Weather and relapses of fungal infection: Ten relapses of plantar fungal infection were photo-recorded from May 1 of 2015 to April 30 of 2018, and all occurred at the hyperkeratosis-like Xiangya lesion. Eight of the ten relapses occurred between October to March, correlating with winter and early spring, and the rest two occurred in August and September of 2017 in a period the subject worked and lived in air-conditioning facilities for more than 20 hours a day. Compared to the 3-year average weather, the 7-day weather during the relapses was higher pressure (p < 0.0005), lower temperature (p < 0.01), rainy day (p < 0.01) and higher humidity (p < 0.025) (Table 1).
Fungal infection and arthritis: Some of the recurrences of the fungal infections were barely noticed and were observed only in the photo records review. In the significant relapses, the infection caused topical inflammatory symptoms, such as red, warm, pain, and swollen, and 3–5 day fatigue, and followed by the onset of arthritis symptoms in days, including stiffness, pain, tenderness and swollen around the joints of fingers, toes, limbs and lumbar (Fig. 1 and 2), and cutaneous nodules on side of finger. Arthritis lasted for the entire course of the fungal infections. Dermatitis and cardiovascular abnormalities concurred with arthritis. Although no anti-arthritis remedy was given, arthritis symptoms faded in a week to two weeks after plantar inflammation subsided.
During the episode of arthritis, the blood monocytes count was elevated at 0.61x109/L during arthritis, and returned to 0.51x109/L, (norm 0.10x109 to 0.60x109/L) in remission. Serum galactomannan (GM) was 0.04. The rest laboratory tests, including the rest of the blood cell count, liver and kidney function tests, rheumatoid factor, anti-CCP antibody, erythrocyte sedimentation rates, and C-reactive protein were all in the normal range during relapses or remissions. The X-ray showed the asymmetric increased thickness of soft tissues on the affected fingers and interphalangeal joints and did not reveal any bone and cartilage deformities on the joints of the hands and fingers (data not shown).
Fungal secreted proteins and arthritis: The amount of fungal secreted proteins for subcutaneous injection was equivalent to 1mL fungal culture medium (either straight medium or 200µL five times concentrated protein solution in PBS, which consisted of approximately 30 secreted protein peptides at a concentration from 0.01 to 1.5µg/mL. The causative protein(s) seemed rather stable as that the protein solution of the injections was stored at 4°C for 14 months and still induced arthritis.
The injections on the front of thighs caused local skin reactions, red, swollen, pain, and tender in areas about 4–8 centimeters in diameters starting in 3–4 hours and lasting for 2–4 days (Fig. 1E). This reaction was similar to the appearance of the skin reaction of the fungal infection or trimming Xiangya lesion. Arthritis symptoms measuring by finger stiffness started in 2–3 days after the initial injection, and in 7–9 days, they quickly improved after the injections ceased (Fig. 3B and C). Once-daily of the injection for nine consecutive days induced arthritis symptoms for 15 days (Fig. 3). Prolonged period injections extended the duration of arthritis accordingly (Fig. 4A). Elevated blood monocytes count, 0.65x109/L, also occurred. The secreted protein(s) that causes arthritis were very potent and should need no more than 2µg/day in each subcutaneous injection, which is 100,000 times less than the amount 200mg of anti-TNFα antibody used one dose per injection in arthritis treatment.
Subcutaneous injections to lab mouse: Before self-experimentation with subcutaneous injections of fungal proteins, 100μL of culture medium from 6 fungal strains’ cultures and fresh medium as control were given subcutaneously to seven groups of three mice in each group for eight consecutive days, and observations continued for ten additional days after the injections. No apparent adverse effect or skin and joint abnormalities resulted from the injections were observed (data not shown).
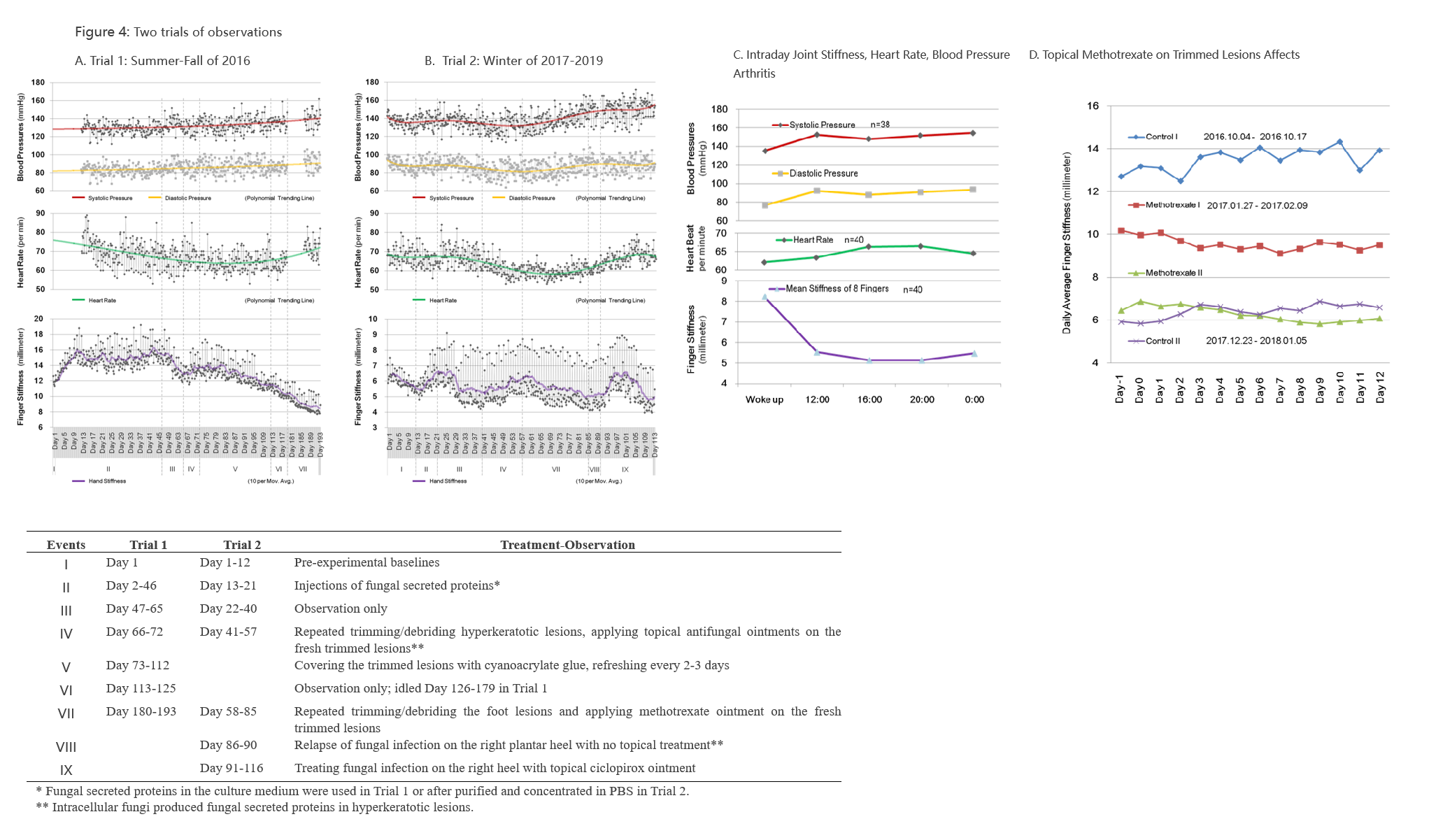
Xiangya lesion and arthritis: Overgrowth of plantar hyperkeratosis-like Xiangya lesion rendered walking pain beneath the lesion and warranted to trim the lesion for pain relief every two months or so. Repeatedly trimming/debriding the lesions led to lesion cell rapid growth and local stimulation sensations for 2–3 days by fungal proteins [11] and followed by the arthritis symptoms in 2 days (Fig. 4D). Topical methotrexate applying twice daily on the lesion immediately after trimming/debriding provided local symptom relief as well as prevented the aggravations of arthritis symptoms (Fig. 4D). Similarly, covering the trimmed lesions with cyanoacrylate glue also had the effect of local symptom relief.
Dermatitis: Dermatitis was a concurrent skin manifestation associated with the relapses of arthritis caused by the fungal infection of the foot and activation of the Xiangya lesion, but it was less apparent when the subcutaneous injection of the fungal proteins was from the cultures. Dermatitis of the skin at the exterior side of the right ankle, above the left knee, the back of finger joints, auricles, and behind auricles gradually emerged following the relapses of the foot fungal infections and arthritis and lasted longer (Fig. 1). The skin started with red and itch, gradually became hyperkeratotic, rough, and pigmented. There were bumpy nodules on or near the arthritic joints, some pain in the active phase of arthritis. Eventually, in months after the arthritis symptoms subsided, peeling skin on dermatitis sites occurred, and the skin returned to a regular appearance in the absence of any topical treatment to dermatitis. Nevertheless, some residual of finger stiffness, dermatitis on the back of fingers, finger nodules, and high blood pressures stayed into the summer and throughout the year.
Cardiovascular abnormalities: Edema, high blood pressure, and bradycardia were found to be associated with skin fungal infections (Fig. 4 A and B). The edema manifested as swollen digital joints, finger stiffness, and pitting edema on the plantar soles, especially in the morning or after a one-hour walk (Fig. 4). Its appearance coincided with arthritis, but lasted longer and became less severe and eventually disappeared in late summer and autumn.
An increase of blood pressure (BP), especially with systolic pressure, was found to associate with foot fungal infection and fungal secreted proteins in the two trials, where the 30-day average BP (systolic/diastolic pressure) increased from 129/83mmHg in the early phase of the first trial (N = 150) to 150/89 mmHg at the end of the second trial (N = 150) over 1.5 years (Fig. 4A and B). The 30 day average of BP was at 147/83mmHg in four months without using anti-hypertension medications after the second trial ended. Systolic pressure increased more than diastolic pressures, which indicated a decrease of vascular compliance for the underlying cause, possibly due to atherosclerosis, maybe, a mechanism similar to that of the nodule formation on the fingers. Nevertheless, more research will need for the cause of hypertension.
The heart rate of the subject gradually decreased from 70–80 beats per minute to below 60 beats per minute in two trials (Fig. 4). It was sinus bradycardia on an electrocardiogram. After the first trial, the daily average of heart rate slowly returned to 65–75 beats/minute (5 measurements/day, seven days) in 4 months, and after the second trial, 65–70 beats per minute (5 measurements/day, seven days) in 4 months and 70–82 beats per minute (5 measurements/day, 7 days) in 8 months with a remission of the fungal infection.
Methotrexate: Topical 0.2% Methotrexate ointment on freshly trimmed hyperkeratotic lesions twice daily for seven days showed slow growth of the lesion, relief of topical irritation and preventing arthritis symptoms induced by trimming/debriding the Xiangya lesions (see Fig. 4 D). Methotrexate might also reduce the arthritis symptoms after applied to the lesions of the fungal infection. However, methotrexate did not seem to cure the Xiangya lesion, to reduce the lesion size in the long term, or to prevent relapses of fungal infection after ceased.
Treatment: Active fungal infections subsided after treatments with lesion debridement and topic antifungal drugs, namely terbinafine, ketoconazole or ciclopirox, with or without methotrexate and achieved remissions in 3–5 weeks. Arthritis and dermatitis had not been treated for their symptoms and were improved after active fungal infection retreated (Fig. 2). All topical drugs, including terbinafine, fluconazole, clotrimazole, ketoconazole, ciclopirox, urea, and salicylic acid ointments, or oral terbinafine and fluconazole did not seem effective in reducing hyperkeratotic lesion size or the relapses fungal infection on the lesions after ceased the medicine. Topical methotrexate and cyanoacrylate glue film were able to alleviate local symptoms and shortened the period of surging arthritis symptoms. Nevertheless, the 14 days average finger stiffness had been decreased from 13.5mm to 6.08mm, about 7.4 millimeters improvement of the stiffness (54.9% decrease) in 14 months from October 2016 to December 2017 (Fig. 4-D), possibly due to oral terbinafine 125mg/day or fluconazole 100mg/day for 45 days, 3 times each regimen in two years, plus topical treatments and frequent caliper finger measurements serving as digital flexibility exercises.






{kind=link}