This study aims to compare screening costs and linkage to care for viral hepatitis B infection in a migrant population with high expected seroprevalences using POCT or standard venepunctures during outreach screening activities.
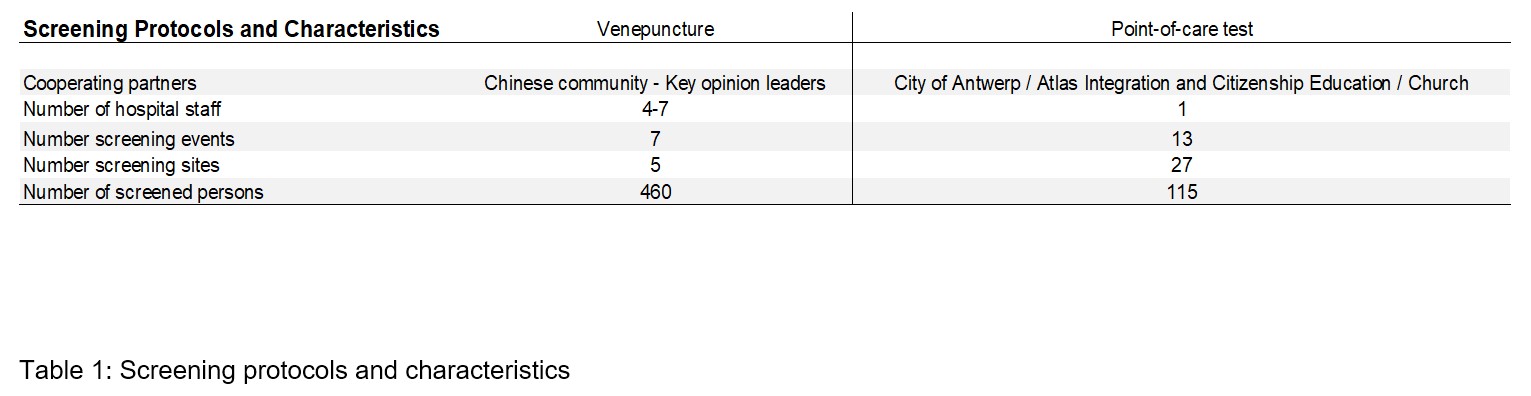
Between 10/2014 and 5/2018, community screening programs were organised with the cooperation of Chinese community leaders, Chinese organisations and the Antwerp City Council. This allowed to screen the same Asian population through multiple angles: during community events in various locations (churches, temples and a local public library in Antwerp and adjacent major Belgian cities), in Asian massage parlours in Antwerp, and through opportunistic testing during mandatory integration classes.
Community leaders, volunteers and screened persons of the Chinese community all participated before, during and after the various screening events. Preparatory meetings were organized to disseminate the rationale of the study, and make arrangements for the logistics of the screening events. A pre-screening questionnaire, communication through written media, social media and word-to-mouth were used. During screening events, community members, translators and Antwerp City Council social workers assisted in logistics and translation services. After screening events, community members also assisted in translation during telephone calls for results and to set up outpatient appointments.
Venepuncture testing for HBsAg was subsequently performed in the Antwerp University Hospital laboratory (Elecsys HBsAg II, Roche Diagnostics GmbH, Mannheim, Germany). POC testing for HBsAg was done with Vikia HBsAg tests (Biomérieux SA, Marcy-l’Etoile, France), according to the package insert. Testing was performed pseudonymised (no personal details were provided but results were given to the screened person) in order to maximise screening uptake in this difficult-to-reach population. Serologic results were given on-site after an incubation time of 15 minutes for the Vikia test, as per the package insert. Upon receiving a positive result, patients were identified and an appointment for specialist care follow-up was immediately agreed upon. POC tested patients’ results were confirmed using standard of care serologic testing (Elecsys HBsAg II, Roche Diagnostics GmbH, Mannheim, Germany) at their first outpatient visit.
Inclusion criteria were: being of Asian descent, first or second generation migrant and birth date before 1999, which is the year of starting universal HBV vaccination in Belgium. Excluded were individuals <18 years old at the screening event and third generation migrants. Minimal clinical data were obtained, after informed consent. Data obtained included: age, gender, nationality, place of birth, HBV infection status, HBV vaccination status, previous or ongoing anti-viral treatment. Results were sent through mail and positively screened persons were notified by phone and also invited for specialist care follow-up.
Additional reflex biochemical (ALT) and virological tests were performed on HBsAg positive samples (HBeAg and anti-HBe antibody: Liaison, DiaSorin, Saluggia, Italy; HBV DNA: in-house method).
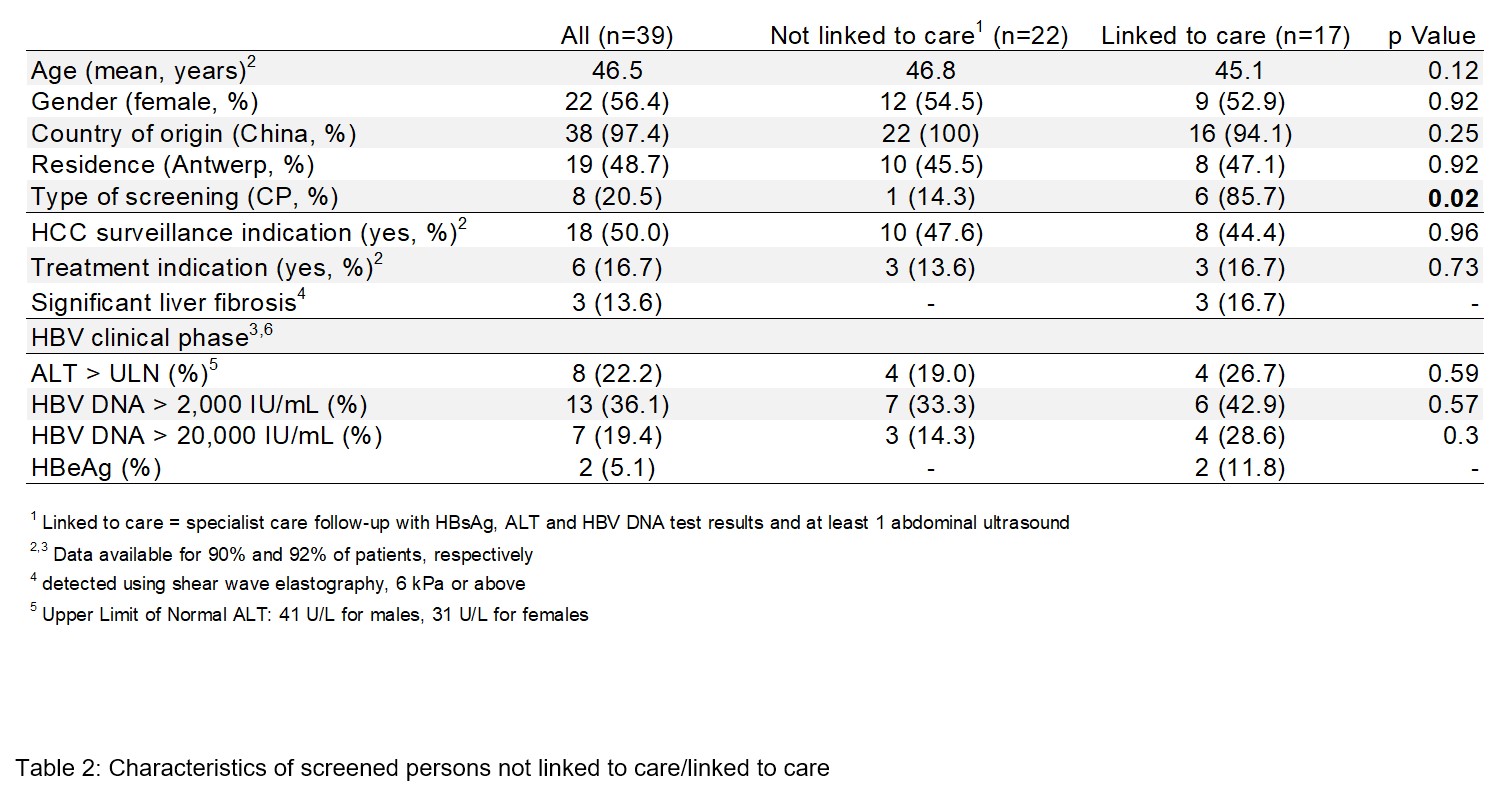
Screening uptake was defined as participating with the screening programs when reached (in any of the described screening events) and providing a valid serological result. Linkage to care was defined as having received specialist care follow-up within 3 months with HBsAg, HBeAg, anti-HBe antibody, ALT and HBV DNA test results, and at least 1 abdominal ultrasound. Analysis of linkage to care was finalised 3 months after the last screening activity by cross-checking positively screened persons and the presence of out-patient clinic patient files at the Antwerp University Hospital. Treatment and HCC surveillance indications were based on international clinical practice guidelines (24,25). All costs associated with the screening activities (personnel, screening tests, other test materials, event-related costs such as fees for screening locations, and communication costs) are listed in euro. Tests performed in the follow-up were excluded, as they were not billed to the patients. Turn-around times, or, the amount of time passed between venepuncture and posting of results in the venepuncture were calculated in days.
Prior to the study, a power analysis was performed to ascertain a valid sample size for seroprevalence of HBV. Previous studies of similar scope (5,6) report a prevalence of HBV infection of 8.5–8.7%. Considering estimates of the Chinese population in Belgium of approximately 13,000–23,000 individuals (17) and extrapolation of 6,239 East Asians in Antwerp city proper in 2014, a power analysis with a precision of 5% (confidence interval of 95%) yielded a required sample size of n = 119.
To determine differences in sampling, seroprevalence of HBsAg between the two screening programs was compared using Chi-square test. To compare screened persons’ characteristics in terms of linkage to care, Student’s T-test was used to compare continuous variables. Chi-square or, where applicable, Mid-P exact test was used to compare ordinal and categorical variables, including the association between screening programs and linkage to care. Given the absence of estimates on differences in linkage to care for both screening programs, no a-priori power calculation thereof was performed.
Statistical tests were performed using SPSS version 24.0 (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.)
{kind=link}
{kind=link}
{kind=link}