The selection of evidence, risk of bias assessment, and meta-analysis were presented according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [19].
All available years of data in PubMed, Physiotherapy Evidence Database (PEDro), and Cochrane Central Register of Controlled Trials (CENTRAL) were searched for potential references. The search strategy used free text word retrieval and subject headings adapted for each database as well as relevant key words such as “ultrasound therapy” and “knee osteoarthritis” with the filter for article type set on “randomized controlled trial (RCT).” The search was conducted until September 2019.
All abstracts identified by electronic database searching were screened by two reviewers to exclude ineligible references. The remaining full articles were then retrieved and screened again for relevance.
The inclusion criteria are as follows:
(1) Randomized controlled trials
(2) Patients with knee osteoarthritis
(3) Studies containing at least one group using LIPUS as an intervention
(4) English literature.
The exclusion criteria are as follows:
(1) Animal studies
(2) Abstract, letter, review, systematic review/meta-analysis, or case report
(3) Non-English literature.
The selected literature was reviewed and evaluated critically by two independent reviewers. The methodological quality assessment was conducted applying the Cochrane Collaboration’s tool for assessing risk of bias[20].
Visual analogue scale (VAS) scores of pain on short and long term were used as outcomes in the meta-analysis. Reviewers extracted all relevant data separately. The extracted and pooled data included first author, year of publication, number of patients, LIPUS intervention duration, observation period, radiation intensity, radiation site, VAS scores, and type of therapeutic exercise.
Meta-analysis was performed using the software package RevMan 5.3, for comparison between LIPUS combined with therapeutic exercise and therapeutic exercise only. Statistical calculations were performed for all studies of interest using detailed LIPUS combined with therapeutic exercise and LIPUS and therapeutic exercise data. The LIPUS group (LIPUS and therapeutic exercise) and the therapeutic exercise group (Therapeutic exercise only) were compared using a random effects model21), significance was considered at P < 0.05. The reliability of the statistic is 95% (confidence interval; CI) was calculated.
Statistical heterogeneity was assessed using I2 statistic[22]. Using a random effects model[11],significance was considered at P<0.05.
RESULTS
In total, 173 potential records were identified through database searches, and 125 abstracts remained after deletion of duplicate records. The abstracts were then reviewed and preliminary assessed, followed by an assessment of the eligibility of 15 full-text articles[23-37]. Of the 15 cases, seven[31-37] met the selective criteria (Figure 1) and the other eight[23-30] were excluded. These eight articles were not eligible for intervention. In addition, three [31,34,35] of the seven articles were used for meta-analysis.
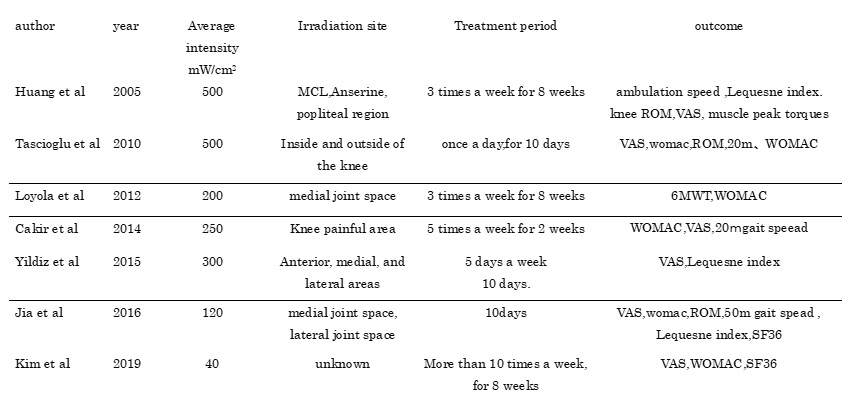
The basic characteristics of included studies are shown in Table 1. The irradiation intensity was 40 ~ 500 mW/cm2, and there was a variation among studies. There was also variation among studies in the area of irradiation, including the medial and lateral cleft MCL, popliteal region, and pain site. Few reports of knee joint function such as muscle strength and range of motion were observed. Figures 2 and 3 show the "risk of bias" assessment for individual studies. Selective bias is unclear because all studies failed to confirm pre-registered outcomes. In one study, the risk of bias increased because patients were not blinded.
We evaluated the efficacy of LIPUS combined with therapeutic exercise for pain compared with therapeutic exercise only, by synthesis of three trials. Pooled VAS score did not demonstrate a short-term effect (MD; -6.86, 95% CI; -18.70 to 4.99 points, I2 = 74%, heterogeneity: P = 0.02) and a long-term effect (MD; -16.01, 95% CI; -32.03 to 0.01 points, I2 = 82%, heterogeneity: P = 0.004) for pain relief with LIPUS combined with therapeutic exercise (Fig 3.4).
{kind=link}