Schummers et al. reported that, compelled by the intuitive appeal of predicting each individual woman’s risk of an adverse outcome, there is a growing interest in risk prediction models [22]. In a systematic review, Al-Rubaie et al. noted that statistical risk prediction models are valuable in identifying women at risk of preeclampsia to guide management, but that specialized models have significantly better performance than simple ones [23]. Importantly, risk-prediction models have been developed in a limited number of settings and there are no such risk prediction models for preeclampsia developed or validated in our low-resource setting at Mpilo Central Hospital or in Zimbabwe. Models developed elsewhere where resources are rich may not be appropriate for our setting as many patients may come from rural settings or have limited antenatal care. Furthermore, risk prediction models developed in rich-resourced settings also use predictor variables such as laboratory markers which are not routinely done in low-resource settings.
Risk prediction models can use routinely collected maternal characteristics to predict risks. Routinely collected maternal characteristics include maternal age, parity, marital status and history of hypertensive disorders some of which are known to be associated with the development of hypertensive disorders of pregnancy. It is important to note that most of the prediction models for preeclampsia focus on maternal outcomes and with no mention on neonatal outcomes.
Ukah et al. concluded that the ability to predict severe early-onset preeclampsia using simple tests could aid in the management of severe preeclampsia and improve outcomes [24]. In low-resource settings, such risk prediction models could help rural healthcare workers predict disease progression and refer patients earlier rather than later in emergency situations.
von Dadelszen et al. produced the best known model to predict adverse maternal outcomes in hypertensive disorders of pregnancy called the fullPIERS model [25]. It was developed for predicting adverse maternal outcomes from 2023 women with preeclampsia using data from tertiary centres in high-income countries(Canada, New Zealand, Australia and the UK), and used maternal demographics, signs, symptoms and laboratory tests as predictors. It had good discrimination with an area under receiver operating characteristic curve (AUROC) of0.88, 95% CI 0.84-0.92, sensitivity 76% and specificity 87%. fullPIERS accurately predicted adverse maternal outcomes for up to 48 hours, a clinically useful period that allows corticosteroids administration, in-utero transfer or induction. It showed both internal and external validities for predicting adverse maternal outcomes within 48 hours for women admitted with preeclampsia at any gestational age. Ukah et al. found that the ability to recognize women at highest risk of complications earlier could aid in preventing these adverse outcomes through improved management [26,27].
The miniPIERS model was developed for low- and middle- income countries using data of 2081 women from Fiji, Uganda, South Africa, Brazil and Pakistan. This logistic regression model was developed to provide a simple, evidence-based tool to identify pregnant women in LMICs at increased risk of death or major hypertensive-related complications. This model included parity, gestational age on admission, headache/visual disturbances, chest pain/dyspnoea, vaginal bleeding with abdominal pain, systolic blood pressure and urine proteinuria [28]. It had good discrimination, albeit lower than the fullPIERS model, with an area under curve of receiver operating characteristic (AUROC) of 0.768, 95% CI 0.735-0.80. However, the sensitivity was much lower at 41.4% and specificity 91.9%. Individual country analysis showed some variation such that South Africa had an AUROC of 0.762, 95% CI 0.702-0.821 and in Uganda the AUROC was 0.656, 95% CI 0.523-0799.
Thangaratinam et al. did a (Prediction of complications in early-onset pre-eclampsia-logistic regression) PREP-L model with data from 946 women from 53 hospitals in England and Wales [29]. The model included: maternal age, gestation, medical history, systolic blood pressure, deep tendon reflexes, urine protein creatinine ratio, platelets, serum alanine amino transaminase and creatinine. The model showed an optimism-adjusted c-statistic of 0.82 (95% CI 0.80 to 0.84) for composite adverse maternal outcomes by 48 hours. The model used estimated fetal weight and liquor volume by ultrasound scan, uterine artery Doppler, cardiotogography findings and administration of steroids for prediction of fetal outcome. Thangaratinam et al. noted that high-resource settings studied preeclampsia risk prediction models have a potential role in triaging high risk mothers who may need transfer to tertiary units for intensive maternal and neonatal care [30], which would still be a laudable goal in the Zimbabwean context.
Onwudiwe et al. used multiple regression analysis to demonstrate that various maternal characteristics such as uterine artery Doppler and mean arterial pressure provided significant independent contribution in the prediction of preeclampsia with a false-positive rate of 10%, the estimated detection rates of early- and late-onset preeclampsia were 100% and 56.4% respectively [31]. As stated earlier, Al-Rubaie et al. validated simple preeclampsia risk models and demonstrated good risk discrimination achieving the highest AUROC (0.76, 95% CI 0.74-0.77) [23].
Ukah et al. found that the most promising prediction was with multivariable models [27].However, von Dadelszen et al. used a multiple logistic regression model that revealed gestational age on admission to hospital (Odds Ratio(OR) OR, 0.91), dipstick proteinuria (OR, 1.31), and mean platelet volume: platelet ratio (OR, 391.0) independently predicted adverse maternal outcomes in preeclampsia [32].
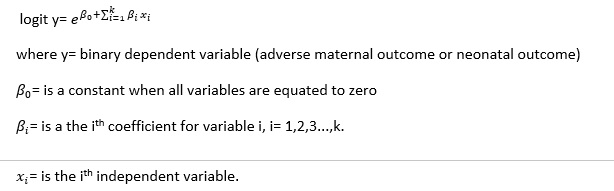
Thangaratinam et al. used logistic regression models to assess the overall risk of any maternal or neonatal outcome and a survival analysis model to obtain individual risk estimates [29]. Other researchers have used statistical models including maternal age, gestation, medical history, systolic blood pressure, deep tendon reflexes, and urine protein to creatinine ratio, platelets, serum alanine amino transaminase, urea, creatinine, oxygen saturation and treatment with antihypertensives or magnesium sulphate. In another example of risk prediction model from a high-resource setting, Gabbay-Benziv et al. found probability scores considering nulliparity, prior preeclampsia, body mass index, diastolic blood pressure and placental growth factor had an AUROC of 0.784 (95% CI=0.721-0.847) [33]. In low-resource settings, due to limited funding in healthcare, some of the biochemical characteristics are not routinely measured hence some cannot be included in the risk prediction models for our locally developed models. Models for low-resource settings e.g. miniPIERS focus on maternal characteristics such as: parity, gestational age on admission, headaches/visual disturbances, chest pain/dyspnea, vaginal bleeding with abdominal pain, systolic blood pressure and urine proteinuria in their model [28].
Almedia et al., validated the fullPIERS and showed an AUROC of 0.72 (p<0.001), determining a cut-off point for fullPIERS probability of 1.7% [34]. In this population, sensitivity of miniPIERS was 60.0% and specificity was 65.1%; the positive likelihood ratio was 1.72 and the negative likelihood ratio was 0.61. The sensitivity implies that 40% of cases of preeclampsia are not predicted at all. The miniPIERS model was well-calibrated and had an AUROC of 0.768 (95% CI 0.735-0.801) with an average optimism of 0.037. Caradeux et al. did a risk prediction model for early-onset preeclampsia with a 5% false positivity and achieving a sensitivity of 62.5% and specificity of 95.5% [35].
The fullPIERS model performed well in the prediction of adverse maternal outcomes in women with preeclampsia but crucially did not attempt to predict neonatal outcome. It is easy to use. The model by Agrawal and Maitra was based on important clinical and biochemical parameters and does not require extensive laboratory testing [36]. This research will develop models for low-resource-settings using patients’ data from Bulawayo to predict risks applicable to patients in a low-resource setting.
This research’s predictor variables will include maternal characteristics, simple bedside and laboratory tests, therapeutic interventions and fetal characteristics similar to the fullPIERS except expensive laboratory tests like detailed renal and liver tests or placental growth factor. It will also be similar to the miniPIERS in terms of low- and middle-income countries settings, but this research will include some basic laboratory tests (haemoglobin, platelets and alanine transaminase) and therapeutic interventions that were not included in the miniPIERS (See Table 1). The model by Thangaratinam et al. was similar in terms of most characteristics but differing in the inclusion of oxygen saturation [29]. Crucially, all these other models only predicted adverse maternal outcome except the one by Thangaratinam et al. This research will predict both adverse maternal and neonatal outcomes in a low-resource setting for the first time using fewer laboratory tests than those done by Thangaratinam et al. due to the difference in the availability of resources [30]. This research will be published as mpiloPIERS, after Mpilo Central Hospital where it is being carried out.
{kind=link}