The introduction of ball-and-spring valves by Nulsen and Spitz in 1949 revolutionized the treatment of hydrocephalus, making conditions with raised ICP surgically treatable16. Although IIH has been treated with shunting for decades, a shift from lumbar to ventriculo-peritoneal shunting has occurred in recent years, mainly thanks to the higher precision allowed by navigation systems. Concurrently, other complications have arisen in patients with CSF diversion. In particular, shunt “overdrainage” has been recognized as one of the most severe consequences of supra-physiologic CSF diversion in VPS. This can lead to small ventricles on imaging, postural headaches and slow refill of the valve reservoir, as well as other neurologic symptoms12. VC can result in Slit-Ventricle Syndrome (SVS), an entity that presents with nausea in the adult population, and premature fusion of cranial sutures with abnormal fibrous tissue and development of secondary craniosynostoses in children. These findings, although frequent among patients with VPS, have rarely been classified into a well-defined clinical syndrome in adult patients, and the limited available evidence for IIH significantly undermines the efficacy of current treatments.
In this study, we aimed to investigate retrospectively in a large cohort of IIH patients treated with ventriculo-peritoneal shunts, the risk factors, clinical and imaging presentation, and treatment outcomes of this therapeutic approach. IIH patients have in fact several characteristics that make them prone to develop VC upon shunting, among which the most prominent are the slit-like appearance and small volume of ventricles at baseline9,10
Further, raised ICP can determine a significant pressure gradient between the ventricles and the peritoneum, increasing the rate of CSF drainage17,18, while the higher distance between the proximal and distal catheters ends in adults makes these devices even more prone to overdrainage than in children.
Risk factors of Ventricular Collapse and their Clinical Importance
Several demographic, radiologic, and vascular risk factors with a role in the development of VC were analyzed. In particular, the use of uni- and multivariate analyses revealed that subjects with smaller ventricles at baseline are more prone to undergo uni- or bilateral VC. This finding, although not surprising from a geometric perspective, is relevant in two ways: first, it raises the hypothesis that abnormally small ventricles result from parenchymal turgor, that also provides a greater force for collapse. Secondly, it suggests the potential use of ventricular size on baseline imaging as a surrogate clinical marker to individuate those patients at risk of developing VC upon shunting.
A possible explanation to the different responses to VPS seen in our cohort could be found in brain turgor19, parenchymal compliance, and the movement of extra- and intracellular water. In support of this hypothesis, the smaller volume of lateral ventricles at baseline could be interpreted as a sign of increased parenchymal turgor, reflecting a stronger predisposition to collapse in patients with IIH and reduced ventricular volume after VPS. In addition, patients with smaller ventricles at baseline experienced a significantly larger decrease in size after shunting, compared to patent ventricles. Patients with VC were found to have a larger decrease in total ventricle area after shunting despite having smaller ventricles pre-procedural (Table 4).
Furthermore, compliance appears to be driven mainly by the displacement and movement of intracranial blood volume, and in particular by its venous component9,14,15,19. Similarly, venous congestion and collapse have been linked to cerebral turgor and distensibility by a variety of studies9,14,19, and appear to be involved in the pathogenesis of IIH and SVS. Consistently with this hypothesis, the ventricular size at baseline may be interpreted as a sign of parenchymal turgor, where smaller ventricles correspond to a larger parenchymal elastic modulus and therefore a higher tendency to collapse upon shunting. VPS in fact, by decreasing the ventricular CSF pressure, reduces the vector counteracting parenchymal turgor and promotes collapse. Further, the lower ICP determined by shunt overdrainage has an indirect effect on cranial veins distensibility, making them more prone to collapse in the supine position, and distended when the patient is standing. The contribution of the venous system therefore becomes an important actor in VC pathogenesis and maintenance, both for its effect on craniocerebral compliance and for the bidirectional effects on CSF dynamics9,20−24. While shunting induces lower pressures in the CSF compartment, venous congestion and sinus/venous stenosis also impact brain distensibility and intracranial volume, potentially modulating the response to treatment and the instauration of a vicious cycle of collapse and re-expansion. Finally, a negative but important finding is represented by the similar distribution of stenotic venous sinuses recorded in the two cohorts, suggesting that the role played by these factors is likely less relevant than previously thought, and that future studies with more sensitive measures are needed to assess their true contribution to the etiopathogenesis of IIH and VC.
Effect of Valve Type and Setting on Ventricular Collapse
Low-pressure valves and shunt overdrainage have been identified as two of the most important risk factors of VC and SVS13, 24–31. For this reason, high OP and programmable valves should be useful in treatment along with the addition of antigravity or antisiphon devices. Programmable valves were used in all subjects, while six patients also received an integrated high-resistance surge-induced alternate high resistance pathway SiphonGuard®).
Although the majority of the valves (64 subjects) were set to a high resistance level of 6 (corresponding to an OP of 18cmH2O) 28 patients (43% of the total) still developed VC. On the other hand, seven patients (7/73) received a programmable valve with SiphonGuard®, and only one experienced VC. These findings suggest that despite the use of programmable valves alone, even at high OP, the occurrence of shunt overdrainage is still a frequent complication. Even high-resistance settings could therefore be insufficient for preventing VC, and the addition of an ASD may improve the flow dynamics and symptomatology. However, our evidence suggests that the ability to increase OP could also reduce the risk of VC and maintain the ventricles dilated in the period after VPS insertion. Although this could cause the persistence of some manifestations of IIH, avoiding the onset of VC might be essential to maintain a normal CSF circulation in the ventricular-subarachnoid, interstitial and transependymal spaces. Furthermore, this could also prevent the onset of a cycle of collapse and re-expansion, difficult to halt once collapse has developed.
Therapeutic Strategies to Reverse Ventricular Collapse
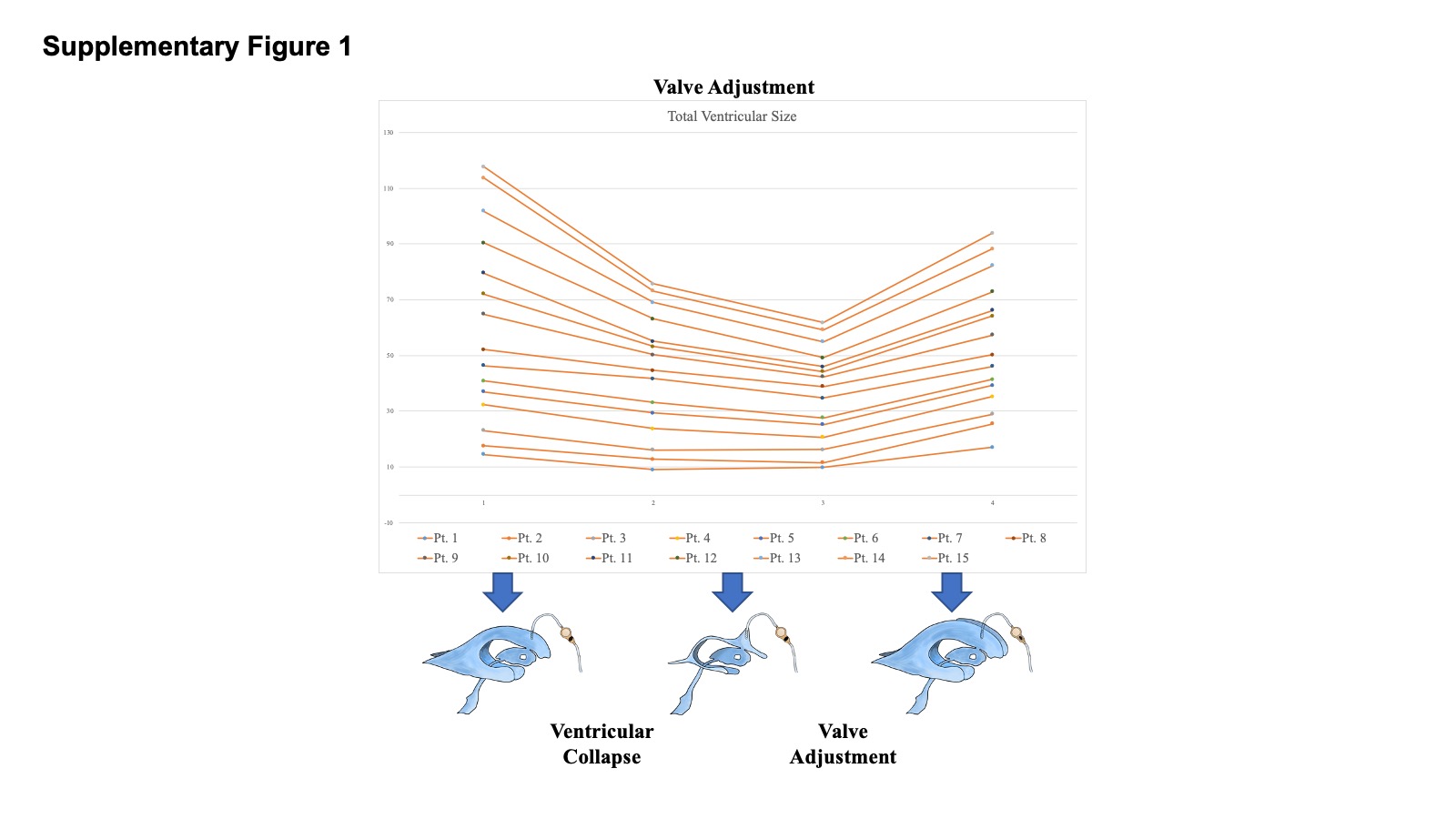
VC is a challenging complication of VPS, usually addressed with an empirical approach, depending on the underlying cause. In some instances, ventricular catheter position is modified or catheters added to drain residual areas of fluid. Unfortunately, this does not address the problem of overdrainage and often results in subsequent collapses. Further, craniospinal disproportion can result in slit and collapsed ventricles and may be best treated with cranial expansion. However, these solutions are not often feasible or first choice of treatment. Valve adjustment appears to be an effective first-line measure in patients with VC, and raising the OP to 21cmH2O or higher achieves radiologic or symptomatic relief in 50% of our cases. In case of failure of this approach, postural overdrainage can be limited by adding an ASD (in our case) to the shunt in use. Although the numbers are small in this series, all the VC patients that were implanted with an ASD after refractory VC experienced complete radiologic and symptomatic resolution. Despite the additional cost and mechanical complexity the use of this shunt adjunct may be justified upfront in all IIH, and strong support to this solution can be found in the literature32–34.
Association of Symptoms and Ventricular Size after Collapse
In this study we found that shunting is usually effective in decreasing headaches and papilledema following the procedure, but these effects can disappear after about six months, both in VC and non-VC subjects (Table 2). Noticeably, unless shunt blockage has occurred, papilledema and ICP remain resolved in patients with the recurrent headaches of IIH, suggesting that other underlying factors might explain shunt-related headaches (Supplementary Table 1).
In our patients that improved after VC only a fraction experienced both symptomatic and radiologic improvement (both headaches relief and ventricular re-expansion). While 10 subjects out of 32 had significantly larger ventricles post-VC resolution on CT/MRI, and 10/32 reported symptomatic improvement, only 9 patients were observed to have both symptomatic and anatomical resolution. It seems clear that the headaches are not directly based on VC and are likely multifactorial. While re-expanding collapsed ventricles may be beneficial from the standpoint of reducing the risk of shunt failure, they are not always associated with the resolution of multifactorial headaches.
Prevention and Treatment of Ventricular Collapse
VC is generally considered an elusive complication of VPS and its pathophysiologic understanding has frequently been framed in the context of SVS in pediatric patients. Nonetheless, the frequency and severity of VC in adult IIH patients deserves a better comprehension and a more extensive use of evidence-based treatments.
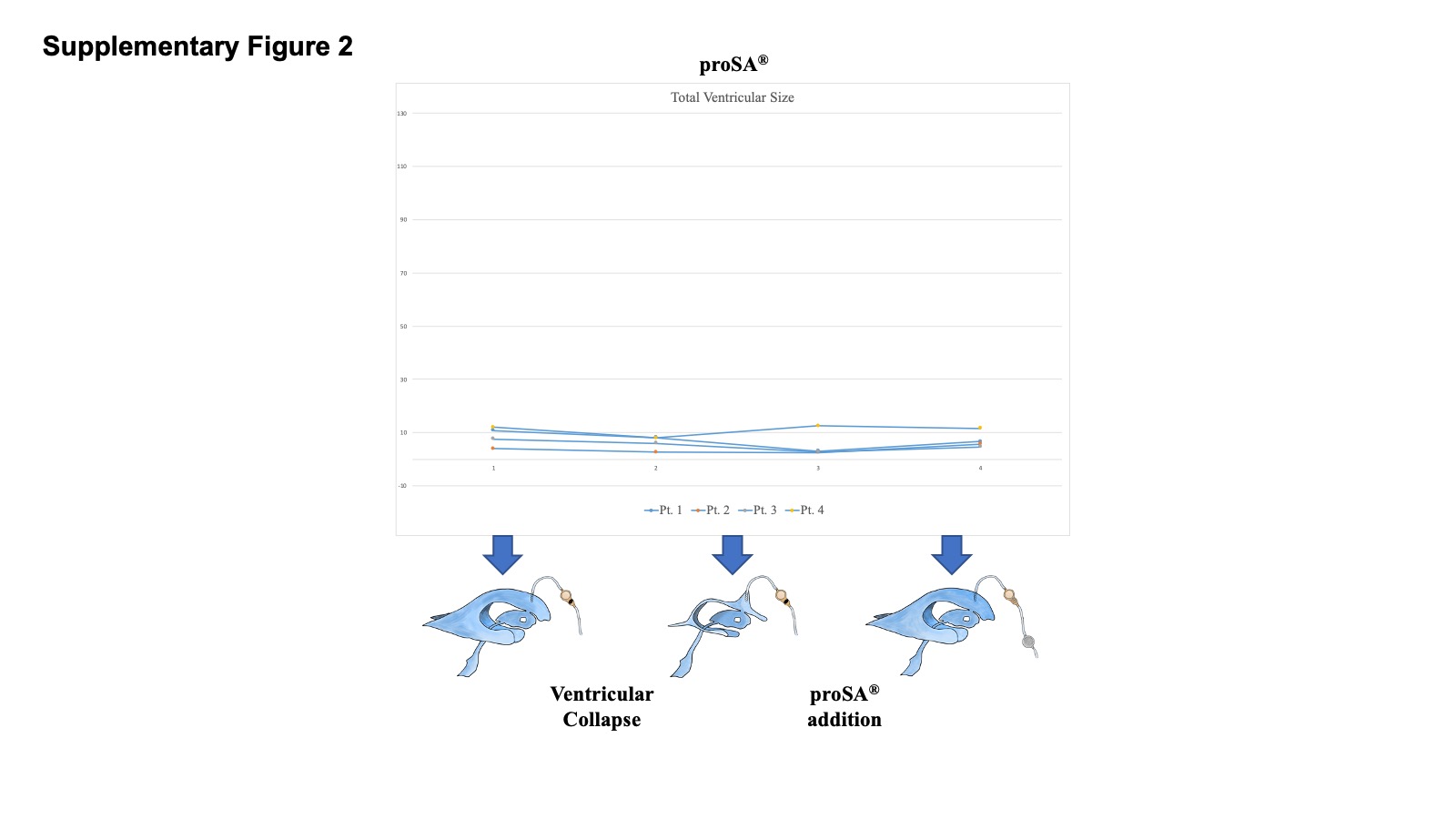
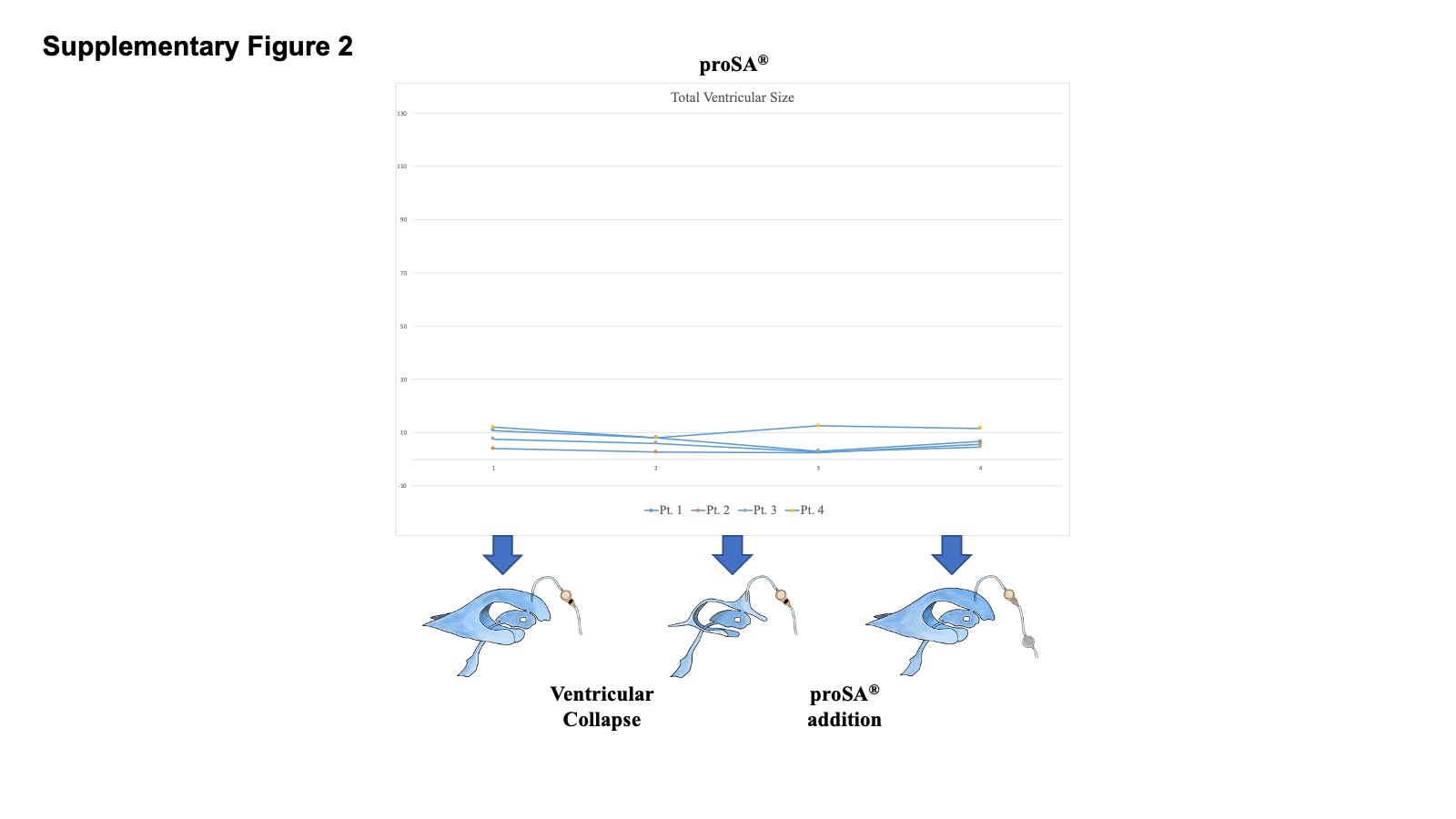
Within the appropriate clinical context, a small ventricular size on imaging (under 9 cm2 of total area) can be a useful indicator of likely VC. Such patients may be provided with a system using a higher OP and the addition of an ASD. Based on our series, VC could likely be prevented by the use of a surge-induced high resistance pathway protector (Siphonguard®) or adjustable gravity device (ProSa®) in the initial shunting of high-risk IIH patients.
Finally, once VC has developed, a number of measures should be taken to induce ventricular re-expansion. First, the valve OP should be raised to a higher resistance, greater than 20cmH2O. This usually allows prompt ventricular re-expansion, despite sometimes resulting in recurrence of IIH “high-pressures” headache symptoms. If this measure fails, the addition of an ASD could reduce postural drainage in presence of symptoms of shunt overdrainage, and improve VC.
Multivariate Linear Regression Models for Predicting Ventricular Collapse
The first multiple regression grouped a number of factors that have been related to the presentation and perhaps etiology of IHH. As a such they may be thought to play a role in the risk of ventricular collapse. Despite their strong association with IIH, papilledema and increased BMI at presentation, and the presence or absence of bilateral transverse sinus stenosis all did not show a significant relationship with development of VC. This may be due in part to the high prevalence of some of these factors in the group and the limited information conveyed by the measurements used (e.g. binomial separation into stenotic/non-stenotic sinuses, subjective classification of papilledema). The significant prediction of ventricular collapse which was observed was largely based on presenting ventricular size. Whether especially small ventricles represent a more severe case of IIH, or just a smaller starting point is not clear. However, an association of small ventricles with increased shrinkage after shunting suggests it was not just the smaller starting point but also a greater driving force that determined collapse.
In the second model, a combination of post-shunting variables (symptoms and area measures) also showed significant association with development of collapse after shunting. As expected, greater decreases in size was associated with VC. However, importantly, the appearance of headache symptoms at six months appeared associated with VC risk and was also found more frequently in patients with VC in the univariate analysis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}