Intensive care beds are expensive and limited. The need for beds varies over time, and sometimes all beds are occupied, particularly on intensive care units (ICUs) where a high proportion of admissions are acute. When a critically ill patient needs admitting to a full ICU, the usual procedure is to either delay admission or create a temporary place for a short period while trying to free an intensive care bed by discharging another patient. This strategy comes at a cost since premature discharge from the ICU to a general ward is associated with increased mortality 1. Transfer to another ICU (ICU to ICU transfer) for various reasons appears to be associated with increased total duration of intensive care and hospital stay, but it is not clear whether this is associated with increased mortality rate 2,3.
Studies on ICU to ICU transfer are problematic since transfers are carried out for three main reasons that must be considered separately in the analyses. First, patients are transferred when there is need for specialised care that is not available in the admitting hospital (clinical transfer). Second, ICU patients are transferred to their home ICU after having undergone initial treatment at another unit (repatriation). Third, patients are transferred to make room for patients with more urgent need for intensive care when all ICU beds are occupied (capacity transfer). Furthermore, follow up of transferred patients should preferably be carried out after discharge from ICU or hospital to capture important long-term effects on survival.
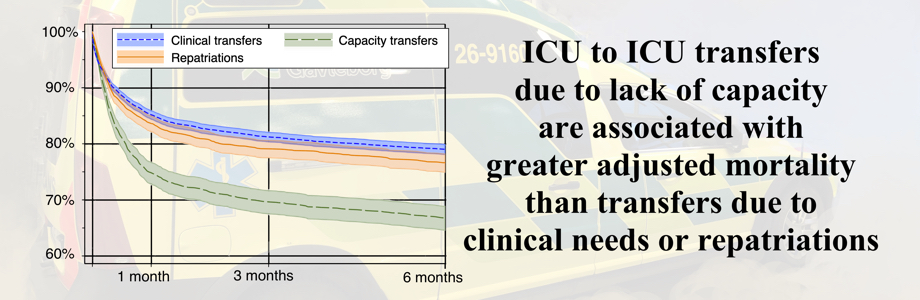
The present study is based on data from a large nationwide intensive care register, the Swedish Intensive Care Register (SIR), which registers the three reasons for transfer named above as well as long-term follow-up data. The hypothesis was that the three classes of ICU to ICU transfer differ in risk-adjusted mortality rate with repatriation having the lowest.
Methods
This was an observational cohort study on patients admitted to Swedish intensive care units (ICUs) from Jan 1st, 2016 to Dec 31st, 2018. Follow-up ended Sept 30th, 2019.
Setting and participants
We used the Swedish Intensive Care Register (SIR) to identify eligible patients (see below). SIR is a national quality register which collects data from intensive care admissions in Sweden. Admissions to a few non-affiliated and paediatric ICUs were not included, leaving data from 75 ICUs for analysis (89 % of all Swedish ICUs). The ICUs were located in local community hospitals (25 ICUs), district general hospitals (24 ICUs) and tertiary care hospitals (26 ICUs).
We included patients (16 yrs. or older) admitted to ICU and subsequently discharged by transfer to another ICU. For patients with multiple admissions during the study period we included the first admission only using the Swedish personal identity number for identification 4. We excluded patients missing to follow-up (i.e. non-Swedes and a few individuals with concealed identity number, n = 714) or missing SAPS3 risk-adjustment data (n = 300 in 4 ICUs).
Variables and definitions
The primary end-point, survival 30 days after discharge from the first ICU, and the secondary end-point, survival 180 days after discharge from the first ICU, were both determined by linking SIR to the Swedish Population Register.
Exposure was discharge to any other ICU (ICU to ICU transfer), whether in the same or in another hospital. Transfers in the SIR are grouped into three categories by the referring intensivist: clinical transfer, capacity transfer, and repatriation. Clinical transfer is where the patient is transferred for specialised treatment or investigations not provided at the first ICU. Capacity transfer is where a patient is transferred to make room for another patient with more urgent need for intensive care when all ICU beds are occupied. Repatriation is where a patient is transferred from the first ICU to another ICU nearer the patient’s home address.
Patient age, gender and admission and discharge times were retrieved from SIR which was the principle data source. The duration of ICU stay was calculated, as well as identification of discharges at night and during weekends. Night time was defined as 10.00 PM to 6.59 AM and weekend as Saturday 0.00 AM to Sunday 23.59 PM 5. We used the Simplified Acute Physiology Score (SAPS) 3 model to score chronic comorbidities and circumstances prior to admission, and reasons for admission and physiologic derangements on admission to ICU 6. The score was subdivided into the original three boxes where Box 1 included comorbidities and time in hospital before ICU (age was deducted from Box1), Box 2 included circumstances on admission, and Box 3 included reasons for admission and physiological derangements on admission. Organ failure at discharge was calculated according to the Sequential Organ Failure Assessment (SOFA) score 7. The score was based on clinical examination before discharge and blood samples obtained on the day of discharge. Missing individual organ scores were presumed normal (0 points). Primary and secondary diagnoses were recorded by the attending intensivist at discharge from ICU according to SIR guidelines. We used the primary International Classification of Diseases version 10 (ICD-10) diagnosis code to group patients into six principal disease groups (See Supplementary Table 1, Additional File 1).
Data were recorded in raw format by each ICU and after local validation transferred to SIR for central validation (required data were present, entries were within prespecified limits, and inconsistencies and illogical entries were identified). If necessary, data were returned for correction and revalidation before being accepted and entered into the master database. In addition to a required comprehensive data set, SIR has a number of optional data sets, including SAPS3 and SOFA, which were used in the present study. While the SAPS3 set was used in all but a few ICUs (300 admissions in 4 ICUs had missing SAPS3 data), SOFA was used in 22 ICUs only. We used admissions from 75 ICUs with SAPS3 data and 22 ICUs with SAPS3 data and SOFA scores at discharge in our risk-adjusted analyses.
Calculations and statistical methods
Descriptive data are presented as mean (95 % confidence intervals, CI) or median (interquartile range, IQR) values and proportions (95 % CI) as appropriate. Differences in crude survival were examined using the Kaplan-Meier estimate and the log-rank test.
The association between category of transfer and survival was analysed using univariable and two-level multivariable logistic regression models (patients nested within ICUs and ICUs treated as a random factor). The primary multivariable model was adjusted for age, gender, comorbidity, reasons for admission, circumstances and physiological derangements on admission as recorded in the SAPS3 model, duration of ICU stay and whether ICU discharge was during the night or weekend. All variables determined by expert opinion and previous experience as relevant predictors of mortality. Additional candidate variables for adjustment were a completely broken down SAPS3 score (instead of the partially broken down score in this study), hospital category, admission time and day of the week.
In a secondary model, in addition to the other variables, the SOFA score was used at discharge using observations from the 22 ICUs using SOFA scores. We performed a sensitivity analysis including admissions with the six principal diagnoses only.
The regression results are reported as odds ratios (ORs) with 95% CI. We used STATA/SE 16 (StataCorp, College Station, TX, USA) for data analysis. A p-value < 0.05 was considered significant. This manuscript is conducted in accordance with the Equator network STROBE-statement 8.
{kind=link}