Long-term complications following COVID-19 are common in hospitalised patients, but the spectrum of symptoms in milder cases remains unclear. In a Norwegian prospective cohort study of 312 patients, 61% of COVID-19 patients (247 home-isolated and 65 hospitalised) had persistent symptoms at six months, most commonly fatigue (37%), impaired concentration (26%), disturbed smell and/or taste (25%), memory loss (24%) and dyspnoea (21%). In young home-isolated adults, aged 16–30, 52% had symptoms at six months, with fatigue (21%), dyspnoea (13%), impaired concentration (13%) and memory loss (11%) posing particular challenges. Pre-existing chronic lung disease and high convalescent antibody titres predicted persistent symptoms, particularly fatigue. Our finding that young, home-isolated adults with mild COVID-19 are at risk of long-lasting dyspnoea and cognitive symptoms highlights the importance of infection control measures, such as vaccination.
Letter
Long COVID affects home-isolated young patients
https://doi.org/10.21203/rs.3.rs-238339/v1
This work is licensed under a CC BY 4.0 License
Journal Publication
published 23 Jun, 2021
Version 1
posted
You are reading this latest preprint version
The COVID-19 pandemic has infected over 100 million people, killed more than two million, and continues to disrupt life across the globe1. While the respiratory tract is the site of SARS-CoV-2 entry and infection, COVID-19 is a systemic disease, affecting the cardiovascular, renal, hematologic, gastrointestinal, and central nervous systems2. As evidence emerges on predominantly lasting impairment of lung function related to fibrosis, this journal has called for more data on the long-term effects of COVID-19 on other organs3. A plethora of symptoms persist in patients surviving severe COVID-194,5, and a long COVID syndrome has been proposed6,7. However, the severity and duration of symptoms remain largely unknown. Chronic fatigue occurred after SARS infection in 2003 8, and it is well-known in the aftermath of a spectrum of infectious diseases, including brucellosis, Q-fever, giardiasis, as well as common viral infections such as influenza, Epstein-Barr virus mononucleosis and dengue fever9-14. It is known from before the current pandemic, that management in intensive care is associated with mental and physical decline, and this could partially explain long COVID in patients with severe illness15. However, the burden of long COVID in mild-to-moderately ill patients is not well known. We assessed persistent symptoms six months following initial COVID-19 illness in a prospective cohort of hospitalised and home-isolated COVID-19 patients from the first pandemic wave in Bergen, Norway.
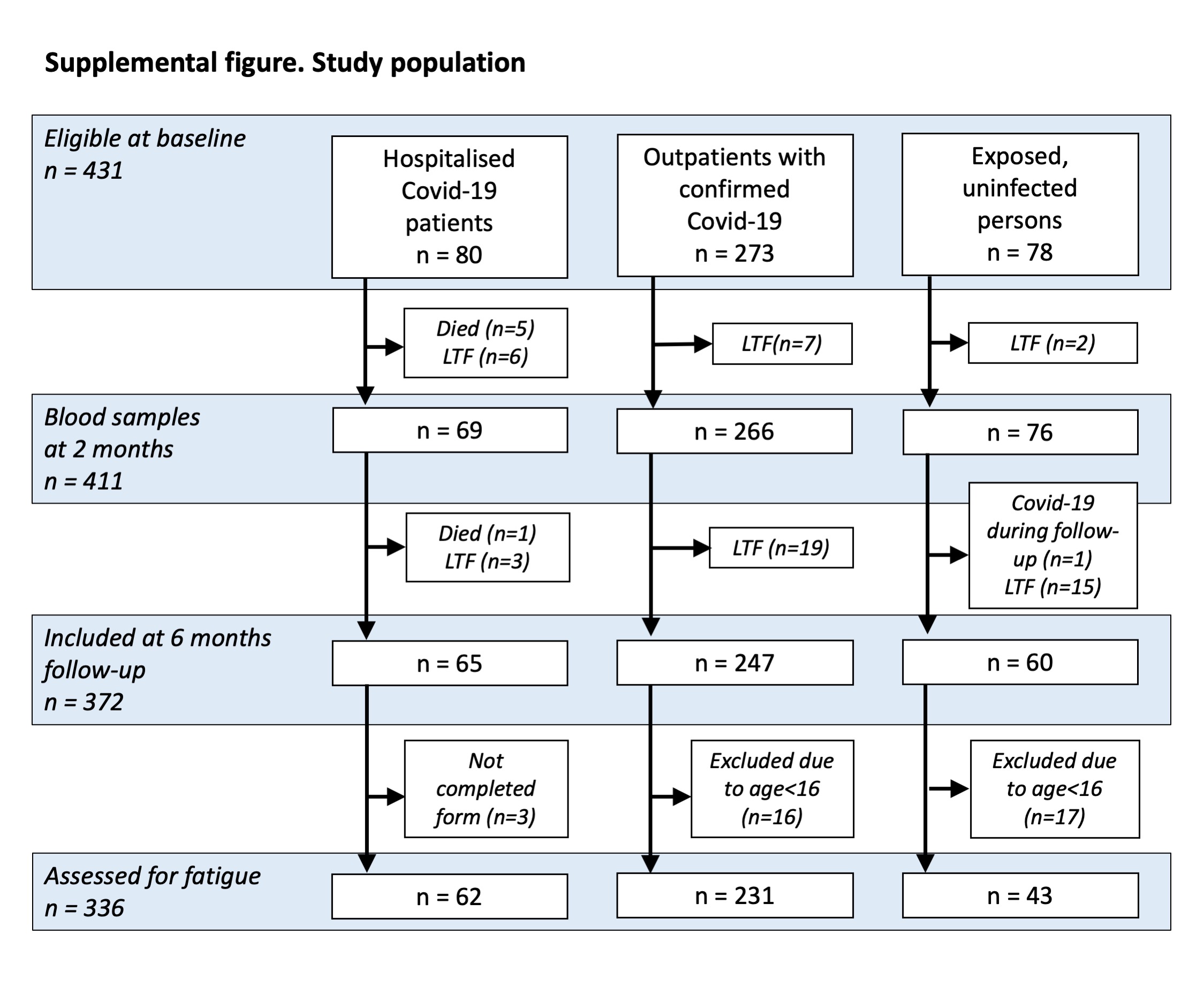
In a prospective cohort study, we consecutively recruited 353 SARS-CoV-2 positive cases from March to May 2020, during the first pandemic wave in Bergen, Norway. We collected demographic and clinical data, as well as blood samples. At six months follow-up, the study population available for analysis comprised 372 individuals, of whom 247 were home-isolated patients, 65 patients had been admitted to the two city hospitals, and 60 were seronegative controls recruited from households of home-isolated patients (Figure S1).
The median age of the COVID-19 patients was 46 years (IQR 30-58), and 48% were male. Forty-four percent had comorbidities, the most frequent being chronic lung disease (12%, 34/38 with asthma), hypertension (11%), chronic heart disease (7%), diabetes (4%) and immunosuppressive conditions (4%). The study population had a median body mass index of 24.6 (IQR[Inter-quartile range] 22.8-27.3). Hospitalised patients were older than home-isolated patients, had higher body mass index (OR [odds ratio], 1.21; CI [95% confidence interval], 1.13-1.31), more comorbidities (OR, 3.79; CI, 2.14-6.94), including chronic lung disease, chronic heart disease, hypertension and diabetes (Table 1). Seronegative controls were younger than COVID-19 patients and had fewer comorbidities.
Sixty-one percent of the total patient population had persistent symptoms six months after initial COVID-19 illness, with the most common complaints being fatigue (37%), difficulty concentrating (26%), disturbed smell/taste (25%), memory problems (24%) and dyspnoea (21%) (Table 2). Seven percent reported cough, while only two percent had persistent fever. Even in home-isolated cases, fifty-five percent experienced persistent symptoms at six months, most commonly fatigue (30%), disturbed taste and/or smell (27%), concentration impairment (19%), memory loss (18%) and dyspnoea (15%) (Table 2, figure panels a1-4). While the youngest age group (0-15 years) rarely suffered persistent symptoms, more than half (52%) of young adults (16-30 years old) who were home-isolated for mild-to-moderate initial illness, had persistent symptoms, the most common being fatigue (21%), dyspnoea (13%) and impaired concentration (13%) and memory (11%). In these young adults, comorbidity was not significantly associated with persistent symptoms (33% vs 31%, p=1) or fatigue (47% vs 27%, p=0.2), although numbers were too small to draw firm conclusions. Whereas the frequency of most symptoms increased with age, disturbed smell and/or taste was more frequent in people < 46 years old (Table 2, figure panel a4).
Convalescent antibodies peak after approximately two months and provide a marker for the magnitude of the immune response. SARS-CoV-2 spike protein IgG and microneutralising antibody titres detected after two months were significantly higher in hospitalised than home-isolated patients (Table 1). In multivariable analysis, both older age (aOR [adjusted OR], 1.009; CI, 1.004-1.014), higher body-mass index (aOR, 1.023; CI, 1.001-1.045) and severity of initial COVID-19 illness (aOR, 1.261; CI, 1.144-1.389) were associated with higher antibody titres at two months follow-up (Table 3, figure panels b1-2, c1-2). Subsequently, high antibody titres were markers of both persistent fatigue (aOR, 1.200; CI, 1.063-1.353) and total number of symptoms (aOR, 1.241; CI, 1.033-1.491, table 3, figure panels b3-4, c3-4). Pre-existing chronic lung disease was also a risk factor for persistent fatigue and total number of symptoms (aOR, 1.294; CI,1.027-1.633), Table 3).
Post-viral fatigue has been reported following the SARS epidemic in 20038 and other viral infections12-14. To assess fatigue, we used the Chalder score, which is validated for adults16,17. Fatigue is defined as a total bimodal score of ≥4 of 11 questions. The presence of fatigue in non-hospitalised COVID-19 reconvalescents was 30%, which was less than in hospitalised cases (63%) but more than in seronegative controls (14%, table 2 and S1). Severe fatigue, defined as bimodal score ≥4 + total ordinal score ≥23, was significantly more frequent in hospitalised than home-isolated COVID-19 reconvalescents (24% vs 7%, OR, 4.02; CI, 1.86-8.64, able S1). In non-hospitalised cases, the most frequent symptoms of physical fatigue (questions 1-7) were tiredness (35%), increased need for rest (30%) and lack of energy (29%), and the most common symptoms of mental fatigue (questions 8-11) were difficulties finding words (23%), difficulties concentrating (19%) and memory problems (18%, table S1).
Female sex, underlying chronic lung disease and severity of initial COVID-19 were independent risk factors for fatigue at six months in binomial logistic regression (Table S2) and zero-inflated Poisson regression (Table 3). Additionally, high convalescent antibody titre was a risk factor for persistent fatigue and for high fatigue score in multivariable analysis (Table 3, figure panels b4 and c4). Increasing age, cardiac comorbidity and use of antibiotics during initial illness, were risk factors for fatigue in univariable analysis, but were not significantly risk factors in multivariable analysis (Table S2).
This study is novel in assessing Long COVID symptoms, not only in hospitalised patients, but also in young patients and home-isolated cases with milder disease. We found that a large proportion of COVID-19 survivors had persisting symptoms six months after initial illness. While it has previously been reported that patients hospitalised for severe COVID-19 frequently suffer long-term symptoms18, we found that more than half of home-isolated, mildly-to-moderately ill COVID-19 patients suffered symptoms six months post-infection. It is alarming that non-hospitalised, young people (16-30 years old) suffer potentially severe symptoms such as concentration and memory problems, dyspnoea and fatigue, half a year after infection. Particularly for students, such symptoms may interfere with their learning and study progress.
The high prevalence of persistent fatigue in COVID-19 patients is striking and appears higher than seen after common infections such as Influenza, Epstein Barr virus mononucleosis and dengue12-14. Data from Norway has previously reported slightly lower chronic fatigue prevalence (11%) in the general population19 than in the present control group (14%). Although this apparent difference may be a coincidence due to small numbers, a higher rate of fatigue in our control group could be due to factors such as stress related to quarantine, worries about sick family members, and the effect of current restrictions on life during lockdown. For comparison, in January 2021, the prevalence of fatigue was only six percent in employees screened before COVID-19 vaccination at our hospital (data not shown). Our finding that females had higher prevalence of fatigue is in line with results from a prior study on the frequency of fatigue in the general Norwegian population19. The association between severity of illness and persistent symptoms is in line with other data from COVID-19 hospitalised patients18. As the respiratory tract is the main target organ for COVID-19, our finding of underlying chronic lung disease (mostly asthma) as a risk factor for persistent fatigue is not surprising. The association of high convalescent antibody titres and fatigue alludes to underlying immunological mechanisms for the fatigue.
The association between severe initial disease and high antibody titres at two months may be due to higher viral load, which could trigger the immune system more profoundly20. The finding of higher convalescent antibody titres with increasing age could be explained by more severe disease in older people, as age is a well-known and strong risk factor for severe COVID-19. However, multivariable analysis indicated that age and severity of illness were independently associated with high antibody titres. This contrasts with reduced antibody responses after influenza observed in the elderly, referred to as immunosenescence.
Our main message is that young, home-isolated adults with mild COVID-19 are at risk of long-lasting dyspnoea and cognitive symptoms. Considering the millions of young people infected during the ongoing pandemic, our findings are a strong impetus for comprehensive infection control and population-wide vaccination.
Study population
As part of a prospective cohort study with long-term follow-up, we enrolled consecutively patients diagnosed with COVID-19 in the period March – May 2020, during the first wave of the pandemic in Bergen, Norway. The study population included SARS-CoV-2 RT-PCR-positive outpatients diagnosed at Bergen Municipality Emergency Department, and those admitted to the two neighbouring city hospitals, Haukeland University Hospital and Haraldsplass Deaconess Hospital. The study was approved by the Regional Ethics Committee of Western Norway (#118664).
Clinical data
All consenting patients provided demographic information, clinical information on symptoms at baseline and six months follow-up, on risk factors including comorbidities, and use of medication. Data was collected on severity of initial illness, i.e. need for hospitalisation, symptoms on diagnosis, need for non-invasive ventilatory support or respirator-treatment. At six months follow-up, all participants aged 16 years or older were invited to complete a validated fatigue questionnaire containing eleven key questions according to the Chalder fatigue scale16,17. Fatigue was defined as a total dichotomised score of ≥4. Severe fatigue was defined as fatigue plus a total Chalder score of ≥23.
Laboratory methods
Diagnosis of COVID-19 was based on RT-PCR on samples from nasopharyngeal swabs and on serological evidence of SARS-CoV-2 antibody positivity21. Convalescent serum samples were collected two months post-infection for detection of anti-SARS-CoV-2 antibody titres and stored at -80°C until analysed. Samples were heat-inactivated for one hour at 56°C before analysis by a two-step ELISA for detecting SARS-CoV-2-specific antibodies to the receptor-binding domain (screening) and the spike protein (confirmation). Endpoint titres were calculated as the reciprocal of the serum dilution giving an optical density (OD) value of 3 standard deviations above the mean of historical pre-pandemic serum samples (n=128)21. Sera with antibodies against the receptor binding domain were tested in microneutralization (MN) assay using the local isolate hCoV-19/Norway/Bergen-01/2020 (GISAID accession ID EPI_ISL_541970) as previously described22. The MN titre is the reciprocal of the serum dilution giving 50% inhibition of virus infectivity.
Statistical analysis
Data was entered using electronic case report forms (eCRF) in REDCap® (Research Electronic Data Capture, Vanderbilt University, Nashville, Tennessee). All analyses were done in R version 4·0·3 (www.R-project.org), and graphs were produced in R using the ggplot and gridExtra packages. Patients who responded to all questions were included in the analysis, and results presented as percentages with means or medians and 95% confidence intervals. Associations with other variables were assessed by Chi square test and binomial logistic regression.
Multivariable analysis was performed by binary logistic regression for dichotomous outcome variables. For convalescent antibody titre as outcome variable, we log10-transformed the titre values to obtain near normal distribution and performed linear regression (Table 3). The outcome variable “number of symptoms”, encoded as integers from 0 to 13, according to symptoms listed in Table 2, had value zero for 39% (123/312) of the observations. Therefore, we employed zero-inflated Poisson regression using the R package “pscl” for multivariable analysis for this outcome variable (Table 3). The Chalder scale for fatigue assessment encompasses values from 0 to 33, with zero as best possible status (“better than usual” on all 11 parameters), and 33 as worst possible outcome (“much worse than usual” on all parameters), and 11 equalling average score “as usual”. A peak of 38% (112/312) of observations were at 12, and only 7% scored lower (range 8-11). For the purpose of multivariable analysis, values from 0 to 12 were recoded as zero, and remaining values transposed by minus 12, to allow for the use of zero-inflated Poisson regression.
Severity of illness was classified using an eight-category ordinal scale, as previously published23. The categories are as follows: 1, not hospitalised and no limitations of activities; 2, not hospitalised, with limitation of activities, home oxygen requirement, or both; 3, hospitalised, not requiring supplemental oxygen and no longer requiring ongoing medical care (used if hospitalization was extended for infection-control or other nonmedical reasons); 4, hospitalised, not requiring supplemental oxygen but requiring ongoing medical care (related to COVID-19 or to other medical conditions); 5, hospitalised, requiring any supplemental oxygen; 6, hospitalised, requiring non-invasive ventilation or use of high-flow oxygen devices; 7, hospitalised, receiving invasive mechanical ventilation or extracorporeal membrane oxygenation (ECMO); and 8, death.
Data availability
Data may be made available upon reasonable request to the corresponding authors. All requests will be reviewed by Bergen COVID-19 Research Group.
Code availability
The R code used to generate all results of this manuscript is available upon request.
Funding: This work was supported by the Trond Mohn Stiftelse (TMS2020TMT05), the Ministry of Health and Care Services, Norway; Helse Vest (F-11628), the Norwegian Research Council Globvac (284930); the European Union (EU IMI115672, FLUCOP, H2020 874866 INCENTIVE); the Faculty of Medicine, University of Bergen, Norway; and Nanomedicines Flunanoair (ERA-NETet EuroNanoMed2 i JTC2016).
- World Health Organization: Timeline: WHO's COVID-19 response. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline. (World Health Organization, Geneva, 2021).
- Gupta, A., et al. Extrapulmonary manifestations of COVID-19. Nature medicine 26, 1017-1032 (2020).
- Meeting the challenge of long COVID. Nature medicine 26, 1803 (2020).
- Zhou, F., et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet (2020).
- Menni, C., et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nature medicine 26, 1037-1040 (2020).
- von Weyhern, C.H., Kaufmann, I., Neff, F. & Kremer, M. Early evidence of pronounced brain involvement in fatal COVID-19 outcomes. Lancet 395, e109 (2020).
- Venkatesan, P. NICE guideline on long COVID. Lancet Respir Med 9, 129 (2021).
- Lam, M.H., et al. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med 169, 2142-2147 (2009).
- Kerr, W.R., Coghlan, J.D., Payne, D.J. & Robertson, L. The laboratory diagnosis of chronic brucellosis. Lancet 2, 1181-1183 (1966).
- Ayres, J.G., Smith, E.G. & Flint, N. Protracted fatigue and debility after acute Q fever. Lancet 347, 978-979 (1996).
- Hanevik, K., et al. Irritable bowel syndrome and chronic fatigue 6 years after giardia infection: a controlled prospective cohort study. Clin Infect Dis 59, 1394-1400 (2014).
- White, P.D., et al. Predictions and associations of fatigue syndromes and mood disorders that occur after infectious mononucleosis. Lancet 358, 1946-1954 (2001).
- Buchwald, D.S., Rea, T.D., Katon, W.J., Russo, J.E. & Ashley, R.L. Acute infectious mononucleosis: characteristics of patients who report failure to recover. Am J Med 109, 531-537 (2000).
- Seet, R.C., Quek, A.M. & Lim, E.C. Post-infectious fatigue syndrome in dengue infection. J Clin Virol 38, 1-6 (2007).
- Geense, W.W., et al. New Physical, Mental, and Cognitive Problems 1-year Post-ICU: A Prospective Multicenter Study. Am J Respir Crit Care Med (2021).
- Chalder, T., et al. Development of a fatigue scale. J Psychosom Res 37, 147-153 (1993).
- Wessely, S. & Powell, R. Fatigue syndromes: a comparison of chronic "postviral" fatigue with neuromuscular and affective disorders. J Neurol Neurosurg Psychiatry 52, 940-948 (1989).
- Huang, C., et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 397, 220-232 (2021).
- Loge, J.H., Ekeberg, O. & Kaasa, S. Fatigue in the general Norwegian population: normative data and associations. J Psychosom Res 45, 53-65 (1998).
- Fajnzylber, J., et al. SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nature communications 11, 5493 (2020).
- Amanat, F., et al. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nature medicine (2020).
- Trieu, M.C., et al. SARS-CoV-2-specific neutralizing antibody responses in Norwegian healthcare workers after the first wave of COVID-19 pandemic: a prospective cohort study. J Infect Dis (2020).
- Beigel, J.H., et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med 383, 1813-1826 (2020).



There is NO Competing Interest.
- SupplFigure1flowchart.jpg
Supplemental figure 1
- SupplTable1fatiguescore.docx
Supplemental table 1
- SupplTable2riskfactorsfatigue.docx
Supplemental table 2
{kind=link}