In this retrospective study, we found increased levels of coagulation activation markers in the plasma of BP patients, after excluding BP patients with cardiovascular disease, or abnormal renal or liver function, which are known to affect the D-dimer and FDP levels. We also detected a positive correlation between D-dimer/FDP levels and BP severity indexes, suggesting the biomarker function of D-dimer and FDP in evaluating BP severity. This would especially be useful in hospitals that do not have access to anti-BP180 IgG tests.
BP mainly affects elderly individuals. During the aging process, inflammation and activation of blood coagulation can be enhanced in BP patients [11]. BP patients can also produce factor V inhibitor, leading to bleeding [12]. All these studies support the correlation between BP and activated coagulation cascade. Our findings revealed that the coagulation cascade was activated in BP and correlated with disease severity and eosinophilia, which are in accordance with a study that estimated blood coagulation in 20 BP patients[13]. The most important clinical consequence of the hypercoagulable state in BP is an increased thrombotic risk, which may account for the cardiovascular event in BP patients. The observation that thrombotic complications occur more frequently in BP patients further supports this viewpoint [14]. Our study revealed elevated plasma levels of D-dimer and FDP in BP patients, further verifying the hypercoagulable state.
FDP has been reported to be involved in cardiovascular diseases. Previous studies have found that FDP participates in the progression of atherosclerosis and thrombus. FDP is also a valuable diagnostic biomarker for patent-type acute aortic dissection patients and thrombosed-type acute aortic dissection patients [15]. D-dimer is a type of FDP which can reflect the degree of coagulation activation and fibrin formation [16]. It was introduced as a diagnostic aid for thrombotic diseases such as pulmonary embolus and deep venous thrombosis [17]. Increased D-dimer and FDP have been reported in many diseases, including Kawasaki disease, aortic dissection, and stroke [17, 7]. A strong correlation between FDP and D-dimer was also reported in many diseases [15, 4, 7]. Here, we also found a similar correlation between D-dimer and FDP in BP.
Elevated D-dimer and FDP may manifest as a generalized inflammatory disturbance in BP. The inflammatory response can induce the activation of blood coagulation both locally, by amplifying the inflammatory network in lesions, and systemically, by leading to a prothrombotic state [18]. In the inflammatory response in BP, eosinophils play a critical role. Our and other studies revealed increased eosinophil numbers in BP [14], which is correlated with BP disease severity [14]. The correlation between eosinophils and anti-BP180 IgG titer suggested systemic inflammation. A positive correlation between the levels of blood eosinophils and D-dimer or FDP suggested a systemic prothrombotic state. This viewpoint is supported by the observed reduction of both D-dimer and FDP levels in 20 responsive patients after immunosuppressive treatment, and their increase in 9 resistant patients.
Eosinophils are known to be a major intravascular location for tissue factor (TF) [19], an initial factor of the extrinsic coagulation pathway. TF can specifically facilitate the early transendothelial migration of eosinophils [19]. In addition, eosinophils can directly damage endothelial integrity by releasing eosinophil granule proteins (EPO) and altering the microcirculation [20]. Eosinophils can also release cationic eosinophilic granular proteins, such as eosinophilic cationic protein (ECP) and major basic protein (MBP), which can neutralize thrombomodulin (highly anionic) via electrostatic binding, finally leading to the inhibition of the thrombomodulin function [21, 22]. In addition, MBP and EPO can activate platelets and promote thrombosis as well [23]. ECP can neutralize heparin and endogenous heparin sulfate, disturbing the anticoagulant function [24]. Thrombin and activated coagulation factors VII and X are proinflammatory mediators, which can induce the production and release of various interleukins, adhesion molecules, selectins, and growth factors, thereby amplifying the systemic inflammatory network [25].
However, we did not find any correlation between eosinophil number and lesion area, which may be because eosinophil numbers are more closely associated with erythematous lesions [26]. Positive correlations among the levels of both D-dimer and FDP, blood eosinophil counts, and lesion area suggest that D-dimer and FDP could be biological indicators of BP disease severity. This viewpoint is supported by the observed reduction of both D-dimer and FDP levels in 20 responsive patients after immunosuppressive treatment, and their increase in 9 resistant patients.
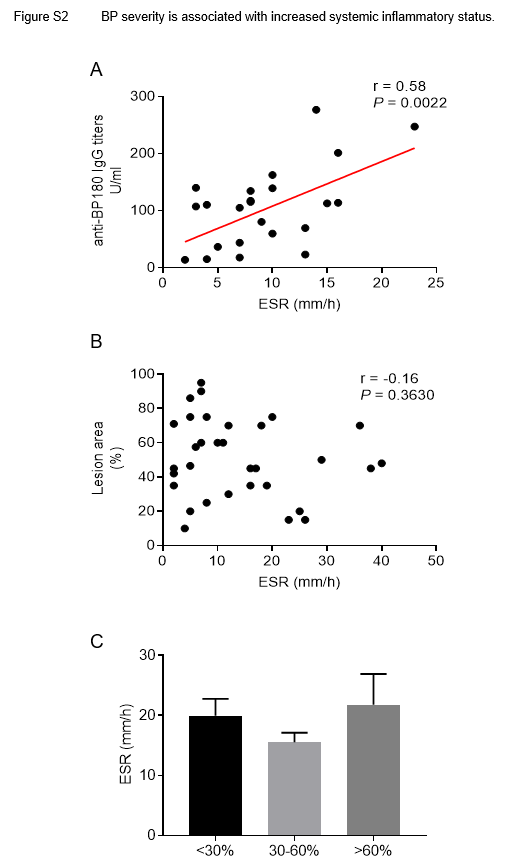
The link between inflammatory response and blood coagulation is further confirmed by a correlation between ESR marker and the hypercoagulable state. Previous findings have shown that an ESR > 30 mm/h correlates with disease activity, and is a risk factor for lethal outcome in patients with Bullous pemphigoid [9]. We found that patients with ESR > 30 mm/h also had higher anti-BP180 IgG titers. Moreover, ESR had a positive correlation with anti-BP180 IgG titers, indicating the potential of ESR in assessing disease severity. We did not find any significant correlation between continuous or dichotomal ESR and lesion area. This may be due to the subjectivity of the lesion area and the non-specificity of ESR. Additionally, patients with ESR > 30 mm/h showed higher levels of D-dimer and FDP, suggesting that increased systemic inflammation may “disturb” coagulation function.
BP is an autoimmune disease mediated by anti-BP180 autoantibodies. The level of anti-BP180 autoantibodies is correlated with BP severity [27] Our study confirmed this correlation. The previous study reported that autoantibodies could also modulate the activation of hypercoagulation [28]. Our results showing that anti-BP180 autoantibody levels correlated with levels of D-dimer and FDP implicated that coagulation could be modulated by autoantibody production, which is in accordance with a previous study [29]. The correlation between anti-BP180 antibodies and eosinophil counts also suggested the role of inflammation. The disturbed autoimmunity probably leads to the production of anti-BP180 antibodies, which then triggers inflammation and promotes the chemotaxis of eosinophils. Eosinophils not only amplify inflammation but also damage blood vessel endothelium, causing a hypercoagulable state in BP.
Our study had a few limitations. Firstly, as the study was conducted in the in-patient department of only one hospital, there may have been choice bias. Outpatients with BP (usually expressing mild symptoms) should be considered in future studies. The selection criteria for the control group were not optimal, as blisters in HZ are usually very limited, and the magnitude of blisters can be milder than that of BP patients. Secondly, based on the selection criteria, only a few patients were included in our study. Therefore, there was a risk of obtaining false-positive results in statistical analyses. Larger sample size and longer collection time are needed to accurately assess the markers to confirm their clinical significance. Thirdly, although convenient, evaluation of the lesion area can be rough, and cannot distinguish among erythema, blistering, and erosion. BPDAI could be a more precise indicator than lesion area of disease severity and could help determine the correlations between lesion types and eosinophils, D-dimer or FDP.
{kind=link}
{kind=link}