The present study demonstrated that PALN dissection for left-sided colon and rectal cancer with synchronous PALN metastasis without other organ metastases was associated with a favorable prognosis. This is one of a few characteristic studies that has shown the clinical significance of PALN dissection.
Similar to liver and lung metastasis, synchronous PALN metastasis from a CRC is categorized as Stage Ⅳ disease. Liver and lung metastasis resection are widely accepted as standard treatments and five-year survival rates are over 50% following surgery.7
PALN dissection was first described in 1950 by Dr. Deddish as a modification of the Miles abdominoperineal resection to reduce local recurrence in rectal cancer.8 However, routine PALN dissection has since been abandoned in view of the increased surgical morbidity, such as urinary and sexual dysfunction, without corresponding improvements in recurrence rates and overall survival.9 On the other hand, recent studies have reported that prolonged survival can be obtained following resection of PALN metastasis.10–14 Each of these studies was a retrospective cohort study, and so significance of the PALN dissection remains unconfirmed and highly controversial.
We think that curative resection, using PALN dissection, is a prerequisite for a favorable prognosis. Past studies have shown that low curative resection rates lead to low survival rates.12 Therefore, we did not perform PALN dissection on patients in whom it was established that curative resection was not possible based on preoperative imaging diagnosis.
Our PALN dissection area was similar to that of past studies. It is necessary to perform PALN dissection for right-sided colon cancer while maintaining the great vessels, such as the superior mesenteric artery or celiac artery. Because of this, in right-sided colon cancer, systematic PALN dissection is anatomically impossible and the dissection effect is not to be obtained as it is with left-sided colon and rectal cancers. For this reason, we limited the indication for PALN dissection to left-sided colon and rectal cancer.
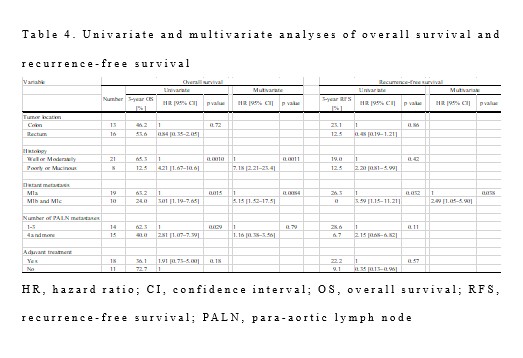
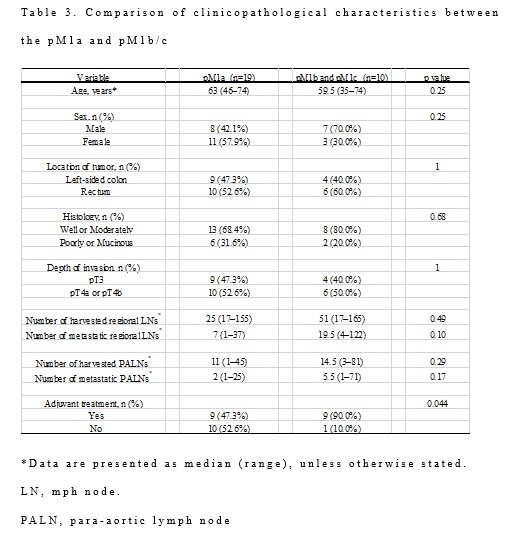
The 3-year OS rate and the three-year RFS rate were significantly better in the pM1a group than in the pM1b/pM1c group, which was similar to the results of Yamada et al.11 In our study, there were no significant differences in clinicopathological characteristics, such as tumor location and histology, the number of metastatic regional lymph nodes, and the number of metastatic PALNs in the pM1a group and pM1b/pM1c group (Table 3). These results suggest that other organ metastases without PALN are the most important prognosticators. In our study, there was no distant lymph node recurrence in the pM1b/pM1c group, and all recurrences occurred in other organs. Consequently, patients with PALN metastasis with other organ metastases should be excluded from the indication for PALN dissection.
Song et al. reported that patients without disease recurrence had three or fewer PALN metastases.14 Several other studies reported that fewer metastases may be a good indication for PALN dissection.2, 15 Speaking of lateral lymph nodes in lower rectal cancer, Fujita reported that the prognosis of patients with one or two extramesorectal lymph node metastases was favorable.16 Our data, however, showed that three patients obtained long-term RFS, even when the number of PALN metastases reached seven or more. Additionally, there are very few reports about the relationship between the number of metastatic PALNs and prognosis, so no influencing factors have been established. Hence, the number of metastatic PALNs cannot guide the indication for PALN dissection at this moment.
Recently, several studies have reported an optimum cutoff for lymph node size to identify patients positive for lateral lymph node metastases of lower rectal cancer on preoperative imaging.17, 18 However, reports on preoperative diagnosis of PALN metastasis are rare. Further studies on accurate preoperative imaging diagnosis and patient selection for PALN dissection are therefore necessary.
The benefits associated with removing PALN metastasis should be weighed up against the risk of morbidity. In the present study, postoperative morbidity occurred in 31.0% of patients, which was comparable with that of other studies (7.8–38.9%).10–14 The main morbidity was surgical site infection, and the rate of Clavien and Dindo classification grade Ⅲ or above was only 10.3%, with no perioperative death. These results suggest that the incidence of postoperative morbidities associated with PALN dissection is within acceptable limits.
There were several limitations to the present study, including the single institutional experience, the small sample size due to the rarity of this metastatic pattern, and the retrospective analysis. The study period was long, lasting over 30 years; and during this time, the optimal indication for PALN dissection and treatment strategy, e.g. chemotherapeutic regimens, would have changed. Additionally, assessment of sexual dysfunction was not performed. A global assessment method, such as the International Index of Erectile Function, should be used for all cases. However, our results clearly showed that favorable prognosis could be expected in select patients with left-sided colon and rectal cancer using isolated PALN metastasis. In light of our results supporting the role of PALN dissection, large and multi-institutional prospective studies are required to overcome these problems.
{kind=link}
{kind=link}
{kind=link}
{kind=link}