Participants and study design
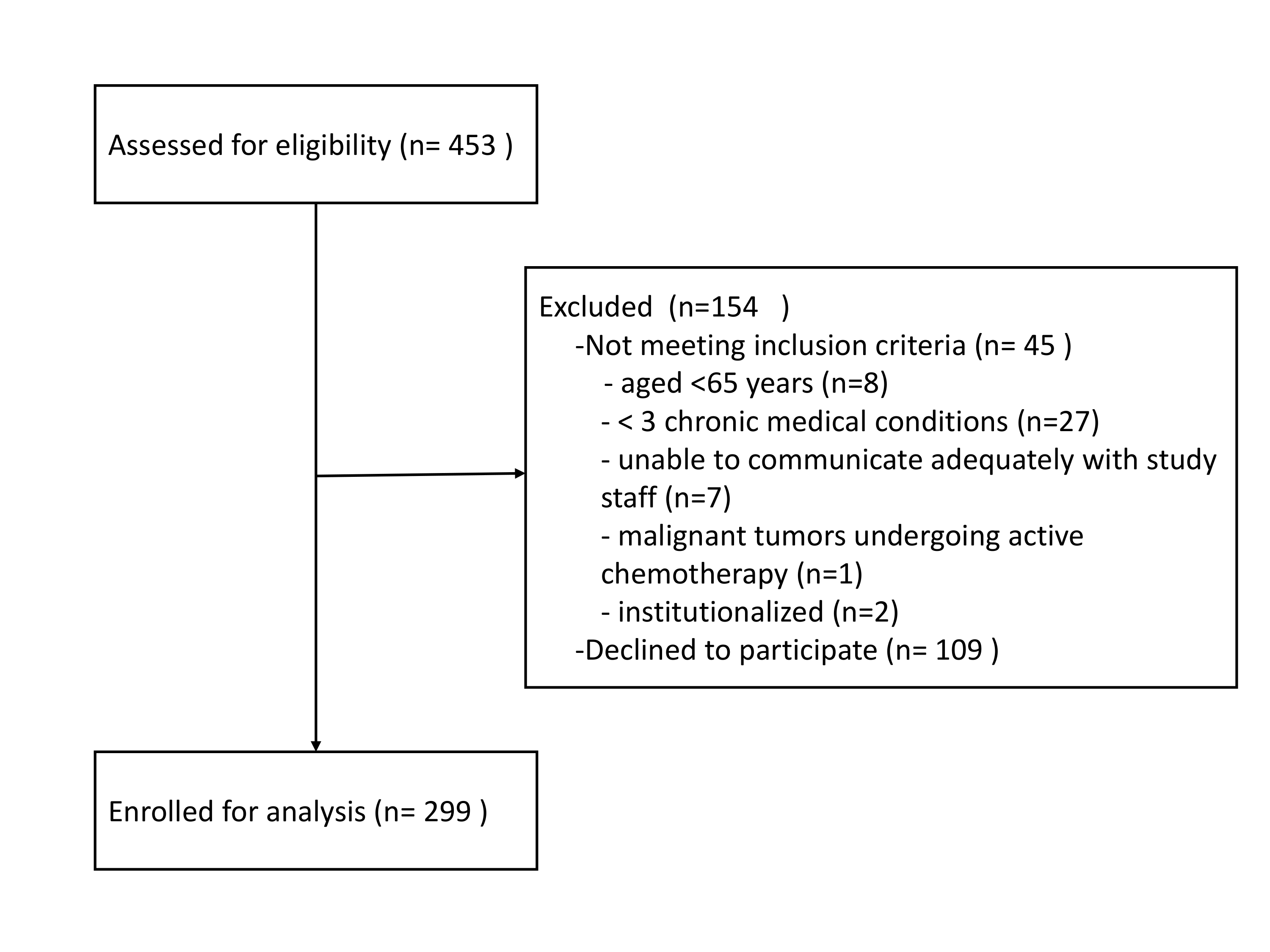
This cross-sectional study recruited older multimorbid community-living adults in New Taipei City, Yi-Lan County, and Hualien County, Taiwan, between July and December 2018. The inclusion criteria were: age ≥65 years and ≥3 chronic medical conditions. The study excluded people who: were unable to communicate adequately with study staff; had malignant tumors undergoing active chemotherapy; with life expectancy <12 months; were institutionalized. Supplementary figure 1 showed details of recruitment process.
This study was designed and conducted in accordance with the principles of the Declaration of Helsinki. The Institutional Review Board of National Yang-Ming University approved the protocol (YM107042F). All participants provided fully informed written consent. The design and reporting format follow STROBE guidelines.[7]
Value-based health metrics
The ICHOM Standard Set Older Person comprises three tiers (Supplementary Table 1).[5]Tier 1, achieved or retained health status, includes: all cause survival; death in a chosen place; and frailty. Participants were asked whether they had expressed a preferred place to die, and frailty was defined as clinical frailty scale ≥4.[8]
Tier 2, treatment burden and complications, includes: falls in the last 12 months; polypharmacy with ≥5 drugs;[9] and participation in decision-making, which comprised confidence in ability to manage their own health, discussion and planning of care, being treated with dignity and respect, coordination of care, and discharge to a chosen place. People in whom of these all components were affirmed were classed as having high participation in decision-making.
Tier 3, long-term consequences of care management and health sustainability, includes: loneliness, defined as ≥35 points on the University of California, Los Angeles (UCLA) loneliness scale;[10, 11] limitation of daily activities (disability), defined as Lawton instrumental activities of daily living scale <8 (most independent);[12] 6-metre walk speed at usual pace, with <0.8 m/ defined as slowness;[13] pain and emotional health measured by the Short-Form Health Survey (SF-36), with pain affecting activities of daily living considered pain, and the criterion for depression being ≥5/9 SF-36 depressive symptoms.[14]
Based on items in Tiers 1, 2 and 3 (Supplementary Table 1), a score ranging from 0 to 10 was derived to represent the value-based health status of each individual; a highest tertile score of ≥8/10 was defined as high value-based health status.
Other variables
Physical performance, anthropometric characteristics, and health-related behaviors of all participants were recorded. Any tobacco or alcohol use in the last 6 months was classed as smoking or drinking, respectively. Exercise was defined as fitness activity for ≥30 minutes at least thrice weekly. Blood pressure, height and body weight were measured by standard procedures; body mass index was calculated as weight in kilograms, divided by height in meters squared (kg/m2). All participants were asked whether they had signed a Do Not Resuscitate order, which is an official agreement registered on national health insurance cards. Cognitive function was measured using The Montreal Cognitive Assessment (MoCA), adjusted by adding one point for those educated for ≤12 years (MoCAadj); MoCAadj ≥26 constituted normal cognitive function.[15] Charlson Comorbidity Index quantified disease severity and comorbidity burdens, with high severity defined as a score of ≥2.[16]
Statistical analysis
All analyses were performed with the SAS statistical package, version 9.4 (SAS Institute, Inc., Cary, NC, USA). A two-sided p-value <0.05 was considered statistically significant. Numerical variables were expressed as mean plus/minus standard deviation and categorical variables as proportions. Descriptive characteristics were compared by Student t test or chi-square analysis, as appropriate. To maximize statistical efficiency, the value-based healthcare score was first treated as a continuous variable, then univariable and multivariable logistic regression analyses were used to investigate associations between corresponding variables and higher value-based healthcare status; p <0.1 in univariable analysis was the entry criterion for multivariable analysis.
{kind=link}