IL-34, M-CSF and CD68+‑TAMs in GC
The expression levels of IL-34, M-CSF and CD68+‑TAMs in GC were investigated. Following immunohistochemical staining (Fig. 1), the densities of IL-34, M-CSF and the number of CD68+‑TAMs were determined and are presented as box plots, including medians and 25th and 75th percentiles. IL-34 and M-CSF were decreased >40% and >95%, respectively, in GC compared to tumour adjacent gastric tissues (p<0.05), whereas CD68+‑TAMs were increased 5.5 fold (p<0.05) (Fig. 1).
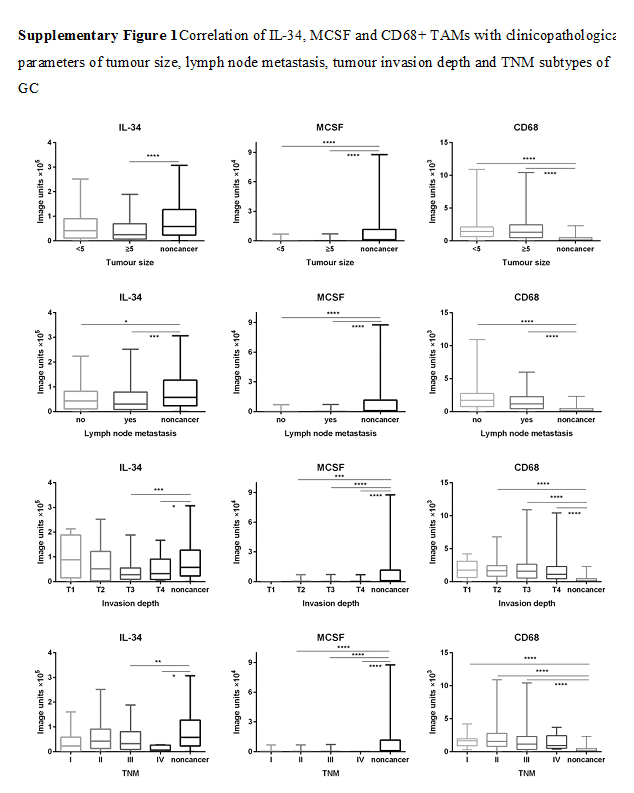
Correlation between IL-34, M-CSF and CD68+‑TAMs in GC and clinicopathological parameters
The median values obtained for IL-34, M-CSF and CD68+‑TAMs expressions were found to significantly differ between subgroups defined by a range of clinicopathological parameters (Table 1, Fig. 2 and Supplementary Figs. 1, 2). The median expression of IL-34 differed significantly with age, gender and tumour differentiation of GC patients (Fig. 2). There was less IL-34 (decreased 46.70%) in the group of patients aged ≤ 60 years compared to patients aged > 60 (p<0.05). Lower IL-34 (decreased 61%) was also observed in female compared to male GC patients (p<0.05). In addition, there was a significant correlation between IL-34 and differentiation of GC (low differentiation group of GC had 74% decreased IL-34 compared to the high differentiation group) (p<0.05), suggesting that IL-34 correlates with the state of differentiation of GC. There was no correlation between IL-34 and other parameters, such as tumour size, lymph node metastasis, tumour invasion depth and TNM stage of GC. Additionally, there was no correlation between clinical parameters and M-CSF or CD68+-TAMs (Supplementary Figs. 1, 2).
Correlation of decreased IL-34, M-CSF but increased CD68+‑TAMs with overall survival of GC patients
To evaluate whether decreased IL-34, M-CSF and increased CD68+‑TAMs correlated with survival of GC patients, low and high cut-off points for IL-34, M-CSF and CD68 were defined by ROC curve analysis (Fig. 3).
The area under the curve (AUC) derived from the ROC curves showed that CD68+-TAM was the most sensitive marker for prognosis (AUC = 0.878), demonstrating a moderate to high accuracy, while IL-34 (AUC = 0.624) and M-CSF (AUC = 0.775) demonstrated only moderate accuracy [22].
Kaplan-Meier analysis was further applied to compare overall survival of GC patients according to combinations of IL-34, M-CSF and CD68+‑TAMs (Fig. 3). Patients with high IL-34 plus high CD68+‑TAMs had the longest survival of GC patients, while those with low IL-34 plus low CD68+‑TAMs had the lowest survival. However, there was no significant difference in survival for the combination of IL-34 and M-CSF, or CD68+‑TAMs and M-CSF.
Furthermore, to determine whether IL-34 was an independent prognostic marker for GC, we performed univariate and multivariate Cox regression analysis, including IL-34, age, gender, tumour differentiation, lymph node invasion, tumour size, the depth of tumour invasion and TNM stage. The effect of IL-34 on patient survival in GC was determined. Univariate analysis (Table 2) revealed that the expression of IL-34, advanced TNM stage, lymph node metastasis, the depth of tumour invasion and tumour diameter were correlated with the prognosis of GC patients. In multivariate analysis (Table 2), only advanced TNM stage remained a significant independent prognostic factor for the survival of patients.
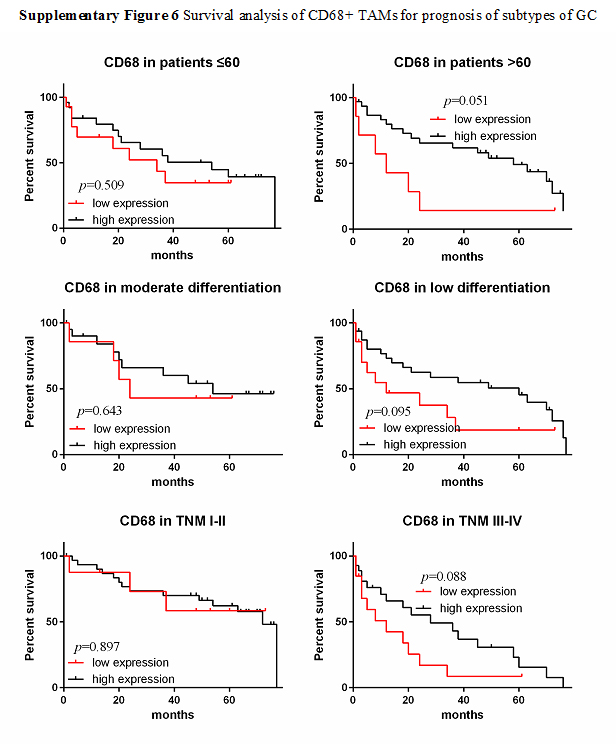
Further analysis of correlation of M-CSF and CD68+‑TAMs with overall survival in subgroups of GC patients
Kaplan-Meier analysis was also applied to further compare overall survival according to M-CSF and CD68+‑TAMs in different subgroups of GC. As results show in Fig. 4, M-CSF correlated significantly with the survival of patients in the TNM III-IV tumour stage. CD68+‑TAMs correlated with survival significantly in male GC patients, larger tumour size (diameter ≥5 cm), lymph node metastasis and tumour invasion depth T3. There was no significance in other subgroups between survival and M-CSF and CD68+‑TAMs (sfig 3-6).
Furthermore, to examine whether M-CSF and CD68+‑TAMs were independent prognostic markers for subgroups in GC, we again performed univariate and multivariate Cox regression analysis, including M-CSF and CD68+‑TAMs, age, gender, tumour differentiation, lymph node invasion, tumour size, the depth of tumour invasion and TNM stage to study the effects of M-CSF and CD68+‑TAMs on patient survival in GC subgroups.
Using univariate analysis a correlation was observed between survival of GC patients and CD68+ TAMs, TNM stage or lymph node metastasis in the T3 stage subgroup of GC patients, respectively (Table 3). Using multivariate analysis, it was demonstrated that CD68+ TAMs and TNM stage remained as significant independent prognostic factors for survival of GC patients within these subgroups.
Using univariate analysis, it was demonstrated that there is a correlation between survival of GC patients and CD68+ TAMs, tumour diameter, advanced TNM stage and lymph node metastasis in the male GC patients’ subgroup (Table 4). Multivariate analysis demonstrated that CD68+ TAMs, tumour diameter ≥5 cm and advanced TNM stage remained as significant independent prognostic factors of survival of male GC patients.
Using univariate analysis for survival in the subgroup of tumour diameter ≥5 cm (Table 5) and lymph node metastasis subgroup (Table 6), CD68+‑TAMs and TNM stage were correlated with the prognosis of GC patients within these two subgroups. However, only TNM stage remained a significant independent prognostic factor of survival of GC patients in multivariate analysis in both subgroups. In the TNM III-IV subgroup of GC patients there was no significant outcome in M-CSF using univariate analysis (sup‑table 1).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}