Method
This was a cross-sectional study in which 300 pregnant women were recruited. The design of this study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (Ref No: IR.AJUMS.REC.1399.006). This study started on 20 March 2020 and completed on 10 April 2020. The oral and written informed consent was obtained from each participant. Literate pregnant women in any trimester of pregnancy were recruited for this study. Women with stressful events in the past 6 months, those with positive test for COVID-19, or those with known mental disorders were excluded from the study.
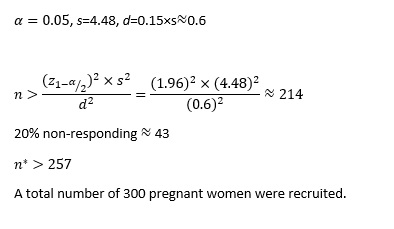
Sample size
The sample size was calculated using the following formula (16):
Measurements
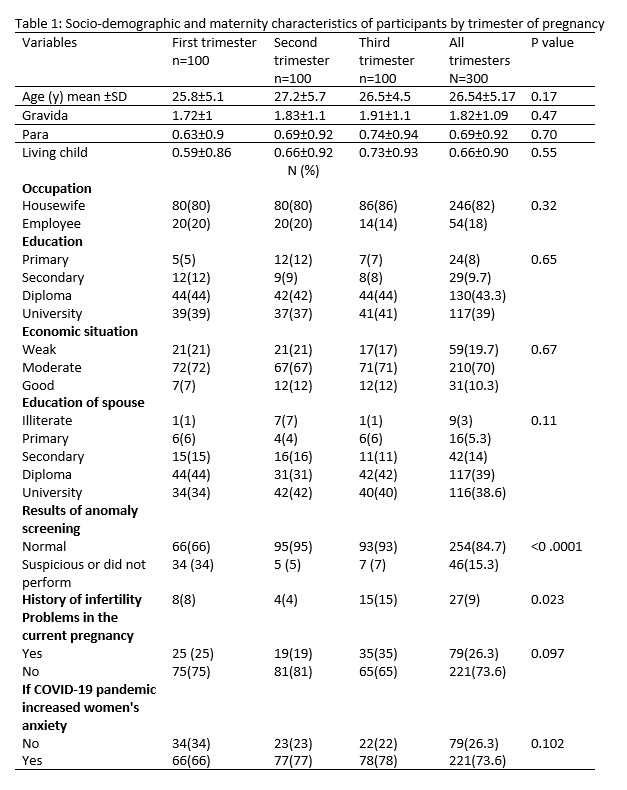
A demographic questionnaire and the Health Anxiety questionnaire were used to collect data. The demographic questionnaire included questions about age, parity, gravidity, number of children, economic situation, the women’s and their partners’ occupation, and the trimester of pregnancy.
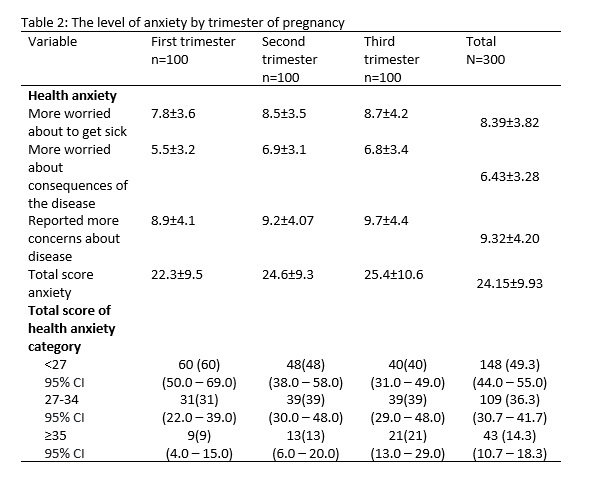
The Health Anxiety questionnaire (17) consisted of 18 questions about the participants’ worry during the pandemic of Corona virus in Iran. Each question had four categories from “I am not worried about my health” to “I spend most of my time worrying about my health”. The score of each item ranged from zero to 3, while zero indicating “I do not have a problem”, and 3 indicating to “I spend most of my time worrying about my health”. The total score of this questionnaire is 54. There are three sub-scales for this questionnaire. The first is related to worry about getting sick, which is reflected in questions 5, 6, 8, 9, 11 and 12. Worry about consequences of disease is the second subscale involving questions 13, 15, 16, 17 and 18, and the third subscale deals with general health concerns, as reflected in questions 1-4, 7, 10 and 14. A total score < 27 means low health anxiety, 27-34 means moderate health anxiety, and scores more than 35 means high health anxiety. The validity and reliability of the Persian version of health anxiety questionnaire had already been assessed and approved in Iran (18). We also included a question asking women if they thought the COVID-19 pandemic had increased their feeling of anxiety during pregnancy.
The phone numbers of pregnant women were obtained from 20 public health centers in Ahvaz. Both questionnaires were sent for eligible pregnant women via social media (WhatsApp or Telegram). The front page of the questionnaires was the written informed consent, and participants were requested to sign this form before responding to the questionnaires. The completed questionnaires were sent back to one of the researchers via the same social media.
Statistics
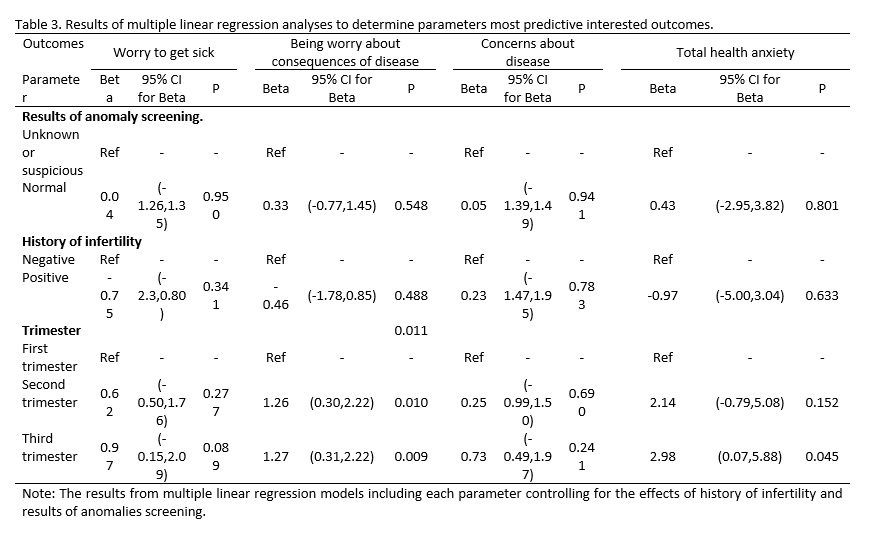
All data were entered SPSS version 22. The normal distribution of continuous data was assessed using the Shapiro-Wilk test. The ANOVA test was used for comparing the data across three groups (three trimesters) and the chi-square test was used for comparing categorical data. Multiple linear regression models were used for assessing the relationship of different trimesters and health anxiety, controlling for the effects of history of infertility and results of anomaly screening. P<0.05 was considered statistically significant.