Research Design and Setting
This quasi-experimental study was conducted with a pretest-posttest two-group design in nursing department of Kerman University of Medical Science in Iran from 2017 to 2019. Kerman University of Medical Science is the biggest university in the Southeast of Iran. The university provides education for undergraduate, postgraduate and PhD nursing students.
Sampling Method
Students were selected by using convenience sampling and were then randomly divided into control and intervention groups by numerical table.
The inclusion criteria included the seventh- and eighth-semester nursing students who were not educated with simulation-based mastery method previously. In addition, students had to pass the theoretical and practical courses such as medical surgical, pediatric nursing, community health nursing, intensive care, psychology-nursing courses.
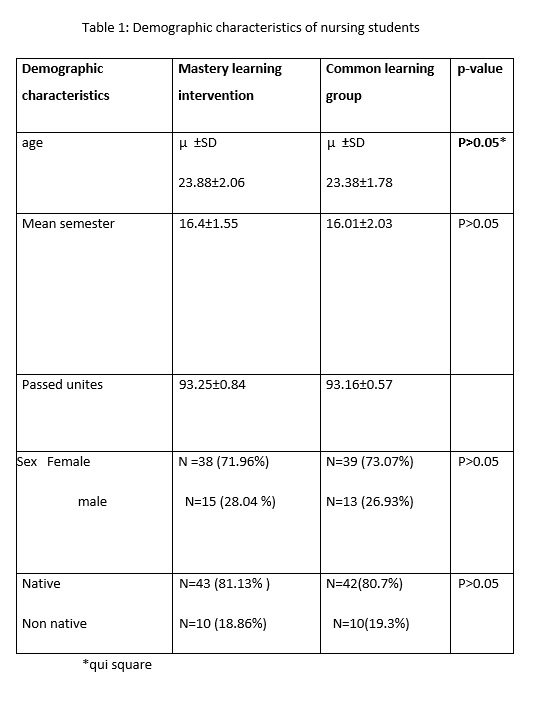
In this study, the research population consisted of 115 eligible BSc students, who met the inclusion criteria. Ten participants were excluded because of absence in training sessions.
In nursing department of KMU, all nursing students had to pass prerequisite courses before taking internship course, including theoretical and practical courses. Theoretical course includes the workshop on patient communication, nosocomial infections, nursing ethics, and a practical course includes common nursing skills trained in proficiency workshop, where advanced special moulage and other equipment are available for nurse students to practice the special nursing skills.
Students will take the practical course after completing the workshops. In addition, taking the internship course depends on passing (80 percent of the checklist) the clinical exam. All students of nursing department had to take the same curriculum.
The research team selected nursing skills commonly used in nursing and agreed on the following four practical skills: suction, nasogastric tube feeding, packed cell transfusion, change of fluid box.
First, the study goals were explained to the participants. The students participated in the study with full consent and agreement. They were explained that attending or not participating in the study would not affect their educational process. The instructors in the two groups completed the demographic characteristic questionnaire and checklist skills before the intervention, and common nursing skills were assessed in two groups by a checklist.
Intervention group procedure
The intervention began on the second day of course. The members of the intervention group experienced a simulation-based mastery intervention in four common clinical skills (suction, nasogastric tube feeding, packed cell transfusion, change of fluid box).
First, the instructor performed each skill on the advanced moulage in proficiency workshop. Then, the students practiced these skills and were assessed by the instructor, who could identify whether the students learned the skill or not (diagnostic feedback) and what they needed to learn better (prescriptive feedback).
A list of student’s mistakes was provided for the relevant instructor and student. The instructors set specific goals for each student based on the deficiencies identified in the first stage. In this program, the instructor used supervisory and observational methods. The instructor observed students and completed checklists every day. The instructor re-evaluated the students through a checklist and re-identified some deficiencies listed in the checklist daily for 12 days (two days a week). In addition, students, who initially fail to demonstrate the skill, have three more opportunities to pass the course. At the end of the course, the clinical skill scores were checked.
To determine the observer's accurate judgment on the examination based on the checklist, two observers assessed the inter-rater reliability of the assessors' scoring for each of the skills. A single-blind method was used, so that the students involved in this study were not informed of the type of teaching methods and how they were placed in each group. In this study, the intervention group experienced simulated mastery learning method.
Control group procedure
Common nursing skills were trained to the students of the control group in proficiency workshop during two sessions a week for six weeks.
The routine teaching method was as follows: the students were divided into groups of three individuals, and clinical skills were performed on the advanced moulage under the supervision of the instructor. In case of any question or mistake, the instructor, a facilitator, would address it. In this method, the instructor taught students according to time-based and summative evaluation with little feedback.
The demographic information questionnaire and the checklist were used in this study to collect the data.
Instruments
The demographic questionnaire contained information about age, sex, scale median, passed credits, grade point average of last semester.
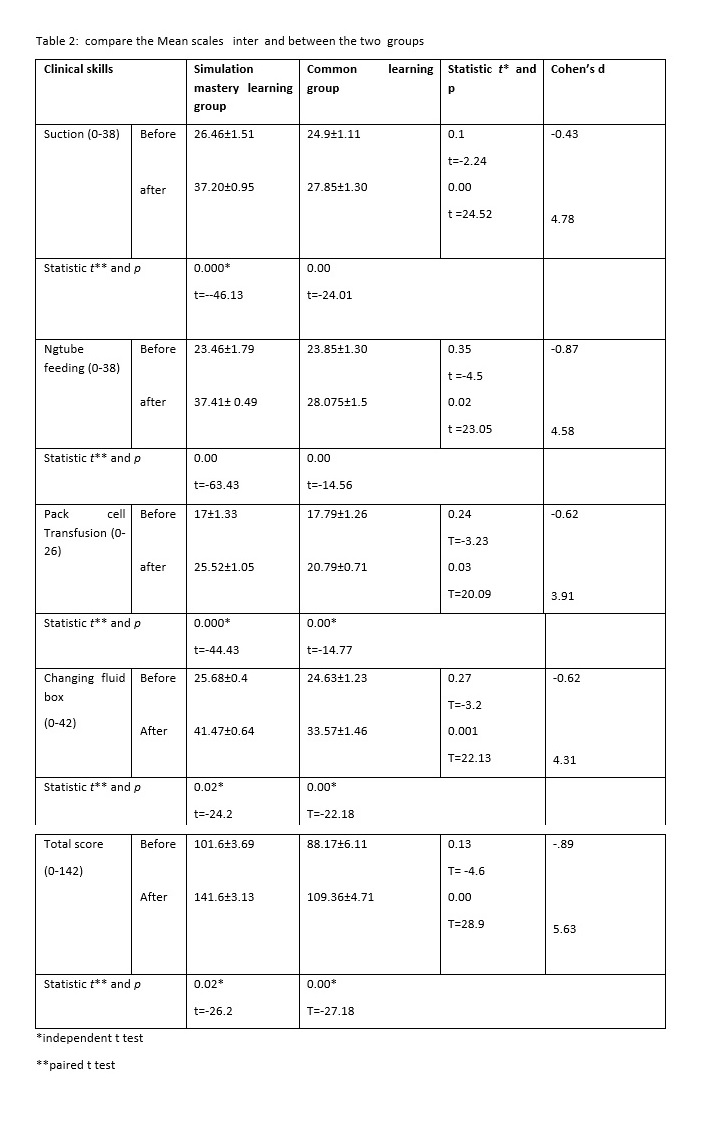
The researchers used four nursing skill checklists for both groups (control and intervention). The checklists were extracted from a nursing book: Skill checklists for Tylor's clinical nursing skills [26]. Suction checklist, the nasogastric tube feeding checklist, the packed cell transfusion checklist, and change of fluid box checklist contain 19, 19, 13, and 21 items, respectively. Each item on the checklists is rated using three scales: unsatisfactory (score: 0), satisfactory (score: 1), and excellent (score: 2). The suction, nasogastric tube feeding, packed cell transfusion, change of fluid box checklists were scored 0-38, 0-38, 0-26, and 0-42, respectively. The total score ranges between 0-144.
The content validity of the checklists was confirmed by the broad consensus, and their reliability was 0.82 by using a pilot study and the Cronbach's alpha coefficient showing a good reliability.
In addition, medical surgical nurses, pediatric nurses and intensive care nurses in Kerman have attempted for five months to prepare and select nursing skill checklists.
Data analysis
The collected data were analyzed using descriptive (frequency, percentage, mean and standard deviation) and inferential statistics. According to the results of the Kolmogorov–Smirnov test, the data of this study had a normal distribution. Thus, parametric tests were used. Furthermore, independent-t test was employed to compare the mean scores of skills between the intervention and control groups before and after the intervention. The paired samples t-test was also used to compare the mean scores of skills in each group before and after the intervention. P-values were considered statistically significant.