FibroTx TAP protein measurements on lesional skin compared to non-lesional skin and healthy volunteers
The skin-surface expression of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 was measured on lesional skin and normal appearing skin of psoriasis patients (N = 30), and on skin of healthy individuals (N =10), using FibroTx TAP tests. Significant differences were observed between measurements of IL-1a, IL-1RA, CXCL-1/2 and hBD-1on lesional skin and non-lesional skin of psoriasis patients, depicted on paired (Figure 1A, panel A-D) and unpaired (Figure 1A, panel E-H) data analyses. The patterns of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 measurements were largely consistent for all patients, but substantial variations were found in expression levels of individual proteins on lesional and non-lesional skin amongst single patients (Figure 1A, panel A-D).
The levels of IL-1a found on lesional skin were remarkably lower than levels found on normal appearing skin; a pattern that was observed in 24 out of 30 psoriasis patients (p < 0.01, Figure 1A, panel E). In contrast, the levels of IL-1RA and CXCL-1/2 detected on lesional skin were notable higher compared to levels found on normal appearing skin of psoriasis patients (p < 0.001 and p < 0.001, respectively) - a pattern that was observed in 26 and 17 of 30 psoriasis patients for IL1-RA and CXCL-1/2, respectively (Figure 1A, panels F and G). The expression levels of hBD-1 found on lesional skin of psoriasis patients were similar to the levels of hBD-1 found on normal appearing skin of psoriasis (Figure 1A, panel H). Biomarker levels detected on healthy apparent skin of psoriasis patients appeared similar to the levels captured on the skin of healthy individuals (Figure 1B, panel A-D). Thus, there is a clear correlation between expression levels of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 and the condition of skin in psoriasis patients.
The inverse expression patterns of IL-1a and IL-1IL-1RA on lesional and non-lesional skin of psoriasis patients, as well as the biological link between IL-1a and IL-1RA, prompted us to analyse the molar ratio between IL-1a and IL-1RA on lesional and non-lesional skin of psoriasis patients. IL-1a and IL-1RA bind to the same receptor, the IL-1 receptor (IL-1R), as a pro-inflammatory agonist and an anti-inflammatory antagonist, respectively. Two forms of IL-1a exist, the immature form with a MW of 31 kDa, and the mature form of 18 kDa, that are both biologically active 36. Both isoforms are recognised by antibodies used for FibroTx TAP. IL-1RA is predominantly expressed as a 17.1 kDa protein 37. The analyses revealed that there is clear molecular excess of IL-1a over IL-1RA on non-lesional skin of psoriasis patients and skin of healthy volunteers, regardless whether IL-1a is present in immature or in mature form, or a combination there-of. Similarly, there is a clear excess of IL-1RA over IL-1a on lesional skin of psoriasis patients regardless of the form of IL-1a (see Table 1).
Correlations between FibroTx TAP protein measurements and psoriasis clinical scores
IL-1a, IL-1RA, CXCL-1/2, are cytokines directly involved in plaque psoriasis skin-inflammation 38-39, which visually manifests itself in the form of redness, thickness and scaling of affected skin 4, 8. A possible explanation for the substantial differences in skin-surface levels of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 on lesional skin of individual patients may be due to differences in disease severity between patients. A clinical method to assess psoriasis severity is the PASI score, which is a weighted score comprised of body surface area affected (BSA) combined with redness, thickness- and scaling of the skin, measured in four different areas of the body (head, trunk, arms, legs) 8 - 9. To assess correlations between FibroTx TAP measurements of psoriatic skin and elements of the PASI score, we analysed the correlation between the values of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 measurements from psoriatic skin against the values (0 - 4 scale) of thickness, scaling and redness at the area of FibroTx TAP measurements, as assessed by a dermatologist. The only statistically significant correlation found was a positive correlation between the clinical score for skin thickness and levels of CXCL-1/2 on lesional skin (see Figure 2 and Table 2).
No statistically significant correlations between measurements of either IL-1a or IL-1RA and any of the clinical scores were detected. Nevertheless, a tendency towards a negative correlation between FibroTx TAP measurements of IL-1a and scaling was observed. The higher the levels of IL-1a on psoriatic lesions, the lower the scaling of lesions (see Figure 2). No apparent correlations were found for FibroTx TAP measurements of hBD-1 from psoriatic skin and clinical assessments of redness, thickness and scaling.
Correlations between FibroTx TAP protein measurements and ultrasound analysis on skin.
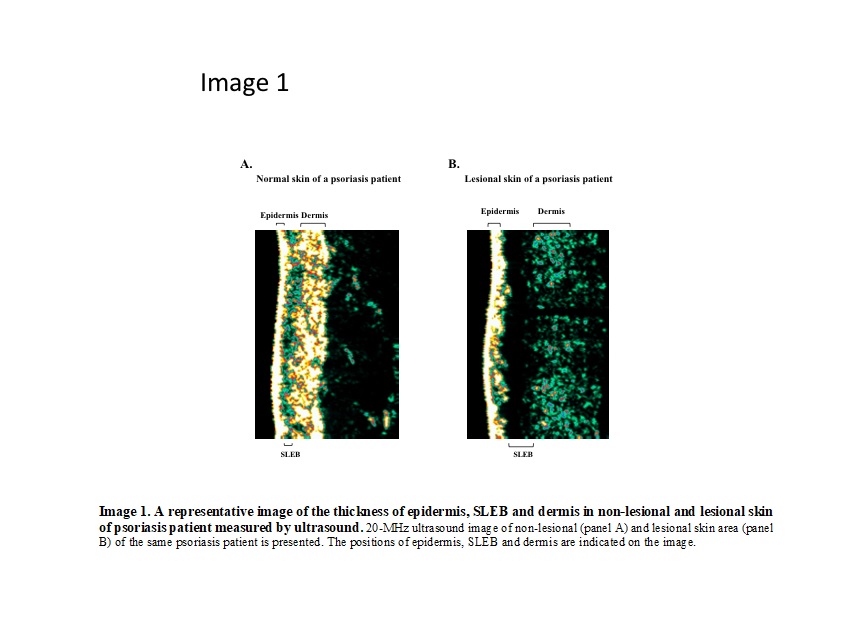
Plaque psoriasis manifests itself in physical changes of the skin layers, such as thickening of the epidermis and presence of a characteristic low-density layer between epidermis and dermis, the so-called sub-epidermal low-echogenic band (SLEB), that can be measured via ultrasound 11-13.
To determine whether differences in the molecular expression patterns of IL-1a, IL-1RA, CXCL-1/2 and hBD-1, between non-lesional and lesional skin site of psoriasis patients correlate with alterations in physical properties of skin layers, FibroTx TAP measurements of these four proteins were correlated with ultrasound measurements from exactly the same skin of psoriasis patients. Using ultrasound, a clear and statistically significant thickening of epidermis (p < 0.001), SLEB (p < 0.001) and dermis (p < 0.001) was measured in lesional skin of psoriasis patients in comparison with non-lesional skin from the same patients (see Figure 3 panel A - C).
Combining FibroTx TAP measurements of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 and ultrasound measurements of normal appearing skin from the same patients did not reveal any strong significant correlations between expression of IL-1a, CXCL-1/2 or hBD-1 and thickness of the epidermis, dermis or SLEB (see Table 3A). A weak positive correlation between IL-1RA and SLEB thickness was observed on non-lesional skin, but not between IL-1RA and epidermis or dermis thickness of lesional skin sites. Combining FibroTx TAP measurements of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 and ultrasound measurements of lesional skin from the same patients also did not reveal any significant correlations between expression of IL-1a, IL-1RA or hBD-1 and thickness of the epidermis, dermis or SLEB (see Table 3B). The only positive correlation was observed between CXCL-1/2 and SLEB thickness on lesional skin. No such correlation was noted between the expression of the CXCL-1/2 and epidermis nor dermis thickness.
To assess whether there are correlations between clinical scores and the ultrasound measurements clinical inflammation scores where correlated with thickness of epidermis, dermis and SLEB analysed at the same skin site. No correlation between skin layer parameters and PASI score was observed whereas positive correlation between lesional skin SLEB thickness and clinical score of thickness (p < 0.05) assessed by doctor was detected (see Table 3C). Among psoriasis clinical scores themselves strong positive correlations between PASI and skin thickness (p < 0.01) as well as between PASI and redness was detected (see supplementary Figure 1) (p < 0.01).
Response to narrow-band UVB treatment measured with TAP
The significant differences between expression levels of IL-1a, IL-1RA, CXCL-1/2 on normal appearing skin and lesional skin of psoriasis patients suggest a strong correlation with disease. Then again, there are no significant correlations between levels of IL-1a, IL-1RA and hBD-1 on skin and quantitative assessments of disease intensity and severity in the form of PASI or ultrasound measurements with the exception of CXCL-1/2 presenting mild positive correlation between skin thickness and SLEB on lesional skin. To assess whether IL-1a, IL-1RA, CXCL-1/2 and hBD-1 are merely qualitative markers of disease, rather than quantitative, we measured expression levels of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 from the skin surface of 14 psoriasis patients undergoing whole-body treatment with narrow band ultraviolet B. FibroTx TAP was used to measure expression of IL-1a, IL-1RA, CXCL-1/2 and hBD-1 on lesional and normal appearing skin of patients before treatment initiation (T0), after two weeks (T1) and after four weeks (T2) of treatment. Treatments were typically performed on three consecutive days in a week. To minimise the risk of measuring UVB-induced inflammation in the skin, rather than measuring the therapeutic effects of UVB on disease, all FibroTx TAP and clinical measurements were performed four days after treatment right before the start of a new three-day UVB-treatment cycle. Measurements were performed on exactly the same position on skin on each time-points. In parallel, visual scores for local inflammation (redness, thickness and scaling) were performed at the exact location of TAP measurements. In addition, the PASI score was determined before and after four weeks of treatment.
As a result of the narrow-band UVB treatment, the PASI score dropped on average 57.71 percent during treatment, a difference that was highly significant (p < 0.001) (see Figure 4A, panel A). Scores for local inflammation (thickness, scaling and redness) showed highly significant improvements of the lesions measured by FibroTx TAP (p < 0.01, p < 0.01, p < 0.01, respectively) (see Figure 4A panel B - C). During the four weeks course of UVB treatment, levels of IL-1a did not change on lesional skin of psoriasis patients, but there was a modest decline in IL-1a on normal appearing skin. In contrast, levels of IL-1RA (p < 0.01) and CXCL-1/2 (p < 0.05) showed a significant reduction on lesional skin in response to narrow-band UVB treatment. Whereas four weeks of treatment reduced IL-1RA on lesional skin to the level of IL-1RA on normal appearing skin before treatment, CXCL-1/2 showed a 75 percent reduction of the level of CXCL-1/2 observed on lesional skin before treatment. No alterations were measured for IL-1RA on normal appearing skin during the course of treatment and CXCL-1/2 remained undetectable. Analyses of the IL-1RA over IL-1a ratio also confirm the clinically observed pattern of normalisation of skin in lesions measured. The ratio between IL-1RA and IL-1a, measured on lesions in apparent concentration (ng/ml) declined from 4.91 to 2.25. In contrast, the ratio between IL-1RA and IL-1a, measured on non-lesional skin remained fairly stable, changing from 0.57 to 0.65 during treatment (see Table 4).
The levels of antimicrobial peptide hBD-1 detected at base line on non-lesional skin are nearly 2 - fold lower compared to the levels captured on lesional skin, however after 4 weeks of narrow-band UVB treatment the levels of hBD-1 detected on non-lesional skin are increased compared to the baseline approximately 2-fold contrary to the levels of hBD1 captured on lesional skin where nearly 4 - fold decrease compared to amounts of base line hBD-1 is detected (see Figure 4B). Due to the UVB treatment the ratio of hBD-1 detected on healthy apparent and lesional skin at base line has changed opposite after 4 weeks.
{kind=link}