The present findings revealed a difference between endoscopic recurrence in the anastomotic site and the causative lesion related to the reoperation. Among other studies presented thus far, Aaltonen G et al. reported that the majority of cases of surgical recurrence (71.4%) were because of a lesion located in the proximal portion of the site of anastomosis and required a new ileocolic resection [3], while other studies also concluded that surgical recurrence after an ileocolic resection is more common in the anastomotic site [4, 5]. Furthermore, the reoperation rate after stoma construction is high in CD patients. In a recent report, Koriche D noted a surgical recurrence rate of 38% with a median follow-up of 2.4 years [6]. Based on these results, step-up therapy based on endoscopic findings of the anastomosis site or oral lesions of the stoma is generally given to affected patients.
In a study performed approximately 30 years ago, Rutgeerts and colleagues showed that the severity of mucosal lesions was correlated with likeliness to develop clinical recurrence [7]. Thereafter, the so-called Rutgeerts endoscopic index has been used to define the primary endpoint in most randomized controlled trials conducted in the recent decade to evaluate preventive strategies for postoperative recurrence (POR) as a surrogate for clinical recurrence. Although POR is usually seen in the neoterminal ileum after ICR, some patients may develop mucosal lesions in another intestinal area. This is not considered when determining Rutgeerts score.
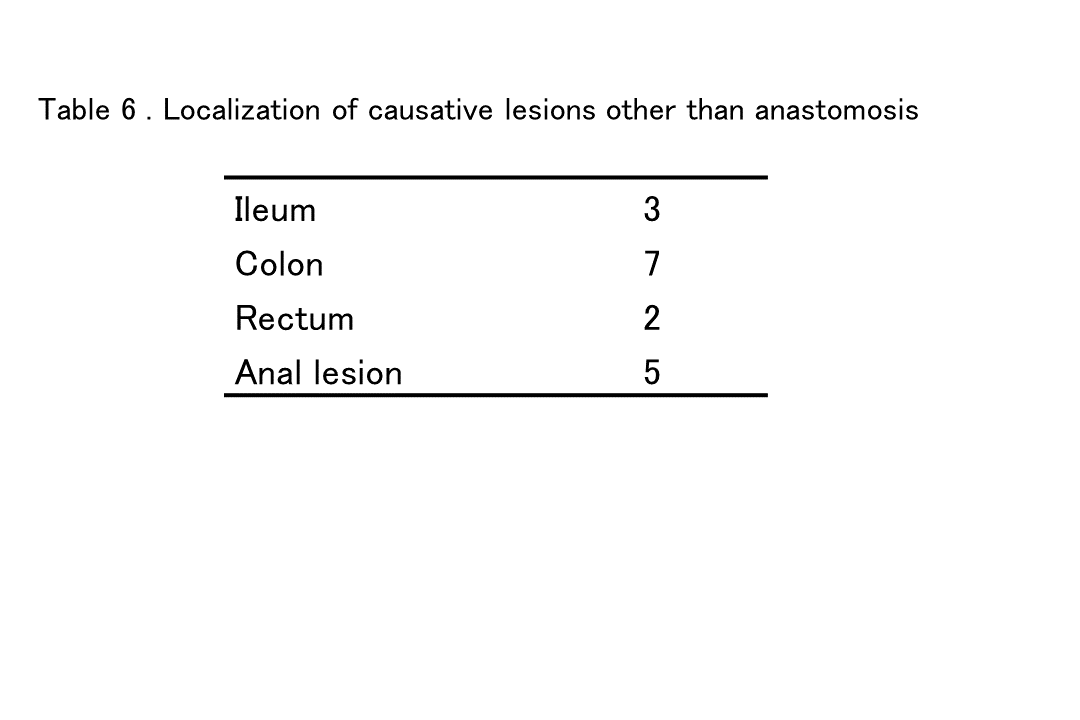
On the other hand, Fichera A et al. noted that even though it is commonly believed that Crohn’s recurrence is always located at the site of a previous intestinal anastomosis, that concept is probably not true and not mindful of the pan-intestinal nature of the disease [8]. In that study, the authors reported that while the site of original operative intervention is the most common for recurrence, as many as one-third of recurrence cases occur in a location separate from that. In the present study as well, 14 (31.1%) cases had lesions away from the anastomotic site that were causative of the reoperation. In addition, abdominal findings obtained at the first operation, even in cases with no macroscopic residual lesions, showed that 9 (29.0%) of 31 of the lesions causative of the need for a reoperation were located in other than the anastomotic region. In the future, an intraoperative lesion search will also require technological progress without relying on the experience and inspection ability of the attending surgeon. In this regard, Celentano V et al. reported the usefulness of an intraoperative ultrasound examination of the small bowel in Crohn’s disease patients [9].
Recently, in order to reduce the number of reoperations caused by anastomosis, improvements in associated treatment methods have been made, with endoscopic balloon dilation of the stenosis site commonly performed. To prevent surgical recurrence at the anastomotic site, Kono et al. developed a new antimesenteric functional end-to-end anastomosis technique in 2003 termed Kono-S anastomosis [10]. With this technique, the supporting column prevents distortion and keeps the intestinal tract in the anastomosis region straight, which also makes endoscopic examination and balloon dilatation following surgery easier to perform. Shimada N et al. reported that the 5-year surgery-free survival rate at the site of anastomosis in patients who underwent Kono-S anastomosis (95%) was significantly higher as compared to those who received an end-to-end anastomosis procedure (81.3%; p<0.001) [11]. Furthermore, in the first randomized clinical trial to compare Kono-S and conventional side-to-side anastomosis procedures in CD patients, Luglio G et al. reported results demonstrating a significant reduction in postoperative endoscopic and clinical recurrence rates for patients who underwent Kono-S anastomosis [12].
Reports of the usefulness of balloon dilatation for stenosis in CD cases are increasing. Shivashankar R noted that endoscopic stricture dilatation in CD patients was safe and effective, and that the most common stricture location was ileocolonic anastomosis [13]. Ding NS as well reported that endoscopic balloon dilatation of an anastomotic stricture in Crohn’s cases is safe and effective over the long term [14]. Based on these results, it is considered possible that lesions in locations other than the anastomotic site will cause a relatively high rate of reoperation.
Alternative non-invasive imaging techniques used to assess postoperative recurrence have been evaluated in recent years [15-17]. Wireless capsule endoscopy has potential advantages over ileocolonoscopy, as it is more comfortable and better tolerated by patients, does not require sedation, and is less influenced by technical limitations. Wireless capsule endoscopy was shown able to detect mucosal lesions one year after surgery in the upper segment of the gastrointestinal tract, outside the area of visualization by ileocolonoscopy, in 60% to 70% of examined patients. Furthermore, in recent years, the number of reports showing the usefulness of minimally invasive magnetic resonance (MR) enterography for evaluation of lesions of CD has been increasing [18, 19].
In future examinations, not only the anastomotic site, but all remaining intestinal tracts should be checked regularly using a minimally invasive method such as capsule endoscopy or MR enterography. In patients with a newly diagnosed lesion, it may be possible to avoid a reoperation by performing step-up therapy.
The present study has some limitations. First, this was a retrospective review of a prospective database of cases experienced at a single center, thus all limitations inherent to a retrospective study apply. Second, the gastroenterologist in charge of the follow-up examinations assessed the need for therapeutic modification on an individual patient basis, without reference to a predefined protocol.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}