Study design, period and area
A community based cross-sectional study design was conducted in Mizan-Aman town, Bench-Sheko Zone, and Southwest Ethiopia from April 16 to May 26, 2020. The town is located 561 km Southwest of Addis Ababa. The town is divided into 5 kebeles that has a total area of 142.71 km with an average elevation of 2840m above sea level. According to the information obtained from the district health office in 2018/19, a total estimated population of 69,453 of which, 32,273 are females. There are one teaching hospital, one health center and five health posts, one University and one college under the government.
Sampling technique and procedure
The sample size was determined by using single population proportion formula with the assumption of 95% confidence level, 5% margin of error and the proportion of behavioral intention towards preconception care use was taken 50% since there is no study previously.
n= (zα⁄2)²*p*(1-p)/d²
Where; n = sample size
Zα/2 = 95% confidence interval (1.96)
P = 50% proportion of behavioral intention towards preconception care use
d = 5% margin of error
Based on the above assumption
n= (1.96)²*0.5(1-0.5) (⁄0.04)²≈384, 10% was added as non-response rate as a contingency rate for the non-response rate. This adjusting for the nonresponse rate/lost or refused to participants during the data collection period is to prevent replacing the non-respondents because replacing is considered as inclusion bias. Let ‘X’ is the expected nonresponse rate and ‘N’ is the number of participants adjusted to prevent replacing the non-respondents because replacing could introduce selection bias. N = 𝑛/ (1 − 𝑥),
N = 384/1-0.1 = 384/0.9 = 426.67 ≈ 427.
So the sample size calculated from single population proportion was 427. Mizan-Aman town was purposively selected then all kebeles (A ‘kebele’ is the smallest administrative unit having 5000 population in average) were taken. To reach the study unit systematic random sampling technique was used in the Kebeles. The first house was selected randomly from 1–24 household and then every 24th house for all kebele was asked(Figure 1). The sampling interval of the households in each Kebele was determined by dividing the total number of households in the specific kebele to the allocated sample size. When there was no reproductive age group woman in the selected house, nearby house was selected and interviewed. In case of more than one eligible woman were encountered in the selected household, a lottery method was used to determine which woman would be interviewed. For the elicitation study, 20 participants were selected by purposive non-probability sampling technique.
Study variables
Dependent variable: Intention to use preconception care
Independent variables:
-
Socio-demographic characteristics:-Age, Religion, Ethnicity, Marital status, Residency, Education status, Occupation
-
Reproductive health related factors: ANC, PNC, FP, planning to pregnancy
-
Knowledge towards preconception care
-
TPB constructs Direct Attitude, subjective norm, perceived behavioral control, indirect subjective norm and indirect attitude.
Data collection process
Pretested interviewer-administered structured questionnaire was adapted from TPB constructs and different literatures 12162122. The questionnaire was developed based on TPB questionnaire development guidelines, different literature and modified based on the result of elicitation study. A face to face interview on 20 persons was conducted to elicit the salient beliefs using open-ended questions. An elicitation study was conducted through in-depth interview to explore relevant salient beliefs among a study population regarding perceived outcome expectation of using preconception care services, perceived social normative influences and beliefs about personal autonomy in seeking the services. Collected data in elicitation study was analyzed using content analysis into themes. The analysis was done by two researchers independently to increase the validity of the analysis. The results from the elicitation study were used to develop a tool for the indirect measurements of TPB constructs by revealing the salient beliefs of each construct. Listing themes in order of frequency for each of the predictors of the TPB model was done. This was done by using Atlas ti 7.0.1 software. Finally, the tool from the themes was prepared for the quantitative study. The questionnaire was prepared first in English and then translated to Amharic and was re-translated back to English by another person to ensure its consistency and accuracy. In addition to constructs of TPB, the questionnaire covered sociodemographic information, knowledge about preconception care and reproductive history. The finally, the overall developed questionnaire was pretested on 5% of sample size before 2 weeks of actual data collection on Tsebejaji town. Four Bachelor science degree holder health professionals were collect data and two health officers were supervising the data collection process. Two days training was given to the data collectors and supervisors on the data collection tools and procedures by principal investigators.
Data management and analysis
The questionnaires were checked for completeness and consistency of data at end to each data collection day. Data were coded, edited and checked for clarity, consistency, and completeness up to the end of the data collection period. The data were coded and entered into Epi-data version 3.1 then exported to SPSS version 25.0 for further analysis. Descriptive statistics were presented in mean and standard deviation for numerical variables and frequency and percentage for the categorical variables. Correlation analysis was conceded out to examine the association between intention and constructs of theory of planned behavior as bivariate analysis. In addition; an independent sample t-test and one way ANOVA was carried out to explore the associations between intention and categorical sociodemographic variables. Those variables which have significant associations with intention to preconception care services at p < 0.25 in bi-variate analysis were qualified for multiple linear regression analysis. Multiple linear regression analysis was conducted to identify independent factors associated to intention to use preconception care service. The “backward” regression technique was used to run the analysis. P-value < 0.05 was considered to indicate significant association.
Each behavioral belief was multiplied by the score for the relevant outcome evaluation to create a new variable that represents the weighted score for behavioral belief. Each normative belief was weighted by each score of motivational to comply and each control belief. Then the weighted beliefs were summed to create a composite score for attitude, subjective norm and perceived behavioral control. Finally, the result was presented and summarized in texts, tables, numbers and figures.
Data quality control
The questionnaire was pre-tested by data collectors in the peoples who do not participate in the actual data collection. Training was given for the data collectors and supervisors on data collection process, approach and with additional training for the supervisors for data quality management. Data collection was closely supervised by the supervisors for the clarity, completeness, and proper procedure of data collection. The questionnaire after data collection was also be checked up by the principal investigator for its clarity and completeness.
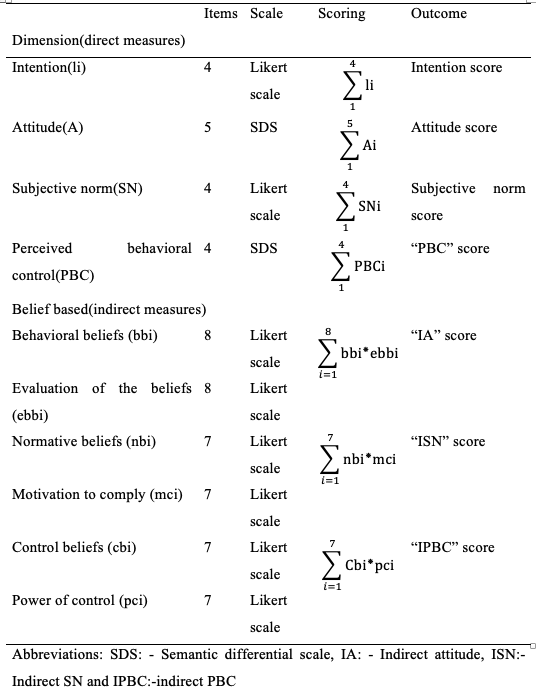
Measurements and Scoring
Intention to preconception care utilization: was measured by using four items. Responses ranged from ‘strongly disagree’ (1) to ‘strongly agree’ (5). Composite score was done by summing up all the items then new composite scores of the intention were created.
Direct attitude towards preconception care use: was measured by 5 items semantic differential scales (SDS) measuring about the benefit/outcome of using preconception care services in the next 3 months on bipolar adjectives. Four Likert scale items were used to measure direct subjective preconception care norm. To assess indirect SN towards preconception care, participants were asked fourteen Likert scale items to indicate the extent to which they thought their health extension workers (HEW), health development army (H.D.A), neighbors, and health workers were likely to appreciate their use of preconception care services. Similarly, the score weighted each normative belief by the score for motivation to comply belief. Then, the composite scores of indirect SN were created by summing up of the weighted beliefs.
Direct measure of PBC was measured by using four items on bipolar differential scales. High composite score shows strong perceived ability or less difficulty to have preconception care services within the specified period of time.
Seven control belief items were used to measure indirect PBC ranging from unlikely to likely scale and perceived power of control was measured using seven items on bipolar Likert scale ranging from ‘strongly disagree’ to ‘strongly agree’. The control belief items were multiplied by those of perceived power of control of the beliefs. Summing up of these product scores yields the composite score of indirect perceived behavioral control. The higher scores indicate a greater value for all measured TPB constructs to towards the use of preconception care services (Table 1).
Knowledge about preconception care utilization were assessed using 17 items with ‘Yes’ or ‘No’ response format23. All items were scored as continuous variables and pulled together where the mean score was computed for further analysis
Practice of preconception care (past experiences): seventeen item was used to ask respondents whether they have ever been practice preconception care by using yes/No approach. Greater than one component use before pregnancy is considered as good practiced11.
Table 1: Summary of measurements and scoring of direct and belief based measures of constructs of TPB of the study conducted in Mizan Aman town southwest Ethiopia, 2020.