Methods
Study design
This is a randomized, single-center, placebo-controlled, double-blinded clinical trial. This research protocol complies with the standard protocol project: Interventional Trial Recommendations (SPIRIT) Guidelines (Additional Document 2). The TH1/TH2 cell polarization index in the serum will be collected to determine the potential impact of people with high PM2.5 exposure. A flowchart of this trial procedure is shown in Fig. 1. This study protocol has been approved by the Chinese Ethics Committee of Registering Clinical Trials (Ethical Review No.: ChiECRCT20190343). Before randomization, all eligible participants will be asked to sign an informed consent (see Additional file 3).
Participant recruitment
We plan to recruit 120 participants from the Chengdu Metro Station. The recruitment methods used in this study include: (1) face-to-face communication, (2) bulletin boards, and (3) posters. We will post recruitment information at various subway stations in Chengdu, and broadcast the recruitment information on the subway broadcast. The members of the research team will receive uniform training after the project is launched, all of whom are medical staff with doctor certificates. The members of the research team will obtain the written consent of the participants, and their mobile phones will be kept open for 24 hours to communicate with the participants at any time. Participants can enter clinical trials only after the members of the research team confirm the qualifications of the participants on the spot and sign a written informed consent form. Eligible participants will be registered and randomly assigned to placebo or omega-3 fatty acids treatment. There is no anticipated harm and compensation for trial participation. All subject personal information and trial data will be treated as confidential, which will be recorded in the individual Case report forms (CRFs). These data will be uploaded in a database that only members of the research team can access. After the later data was completely uploaded, the subjects can enter the website (http://www.medresman.org.cn/login.aspx) to check. Enrollment will begin on November 1, 2020 and is expected to be completed by July 31, 2021.
Sample size
G*Power 3.1 will be used to calculate the sample size necessary to have sufficient statistical power [26]. The sample size calculation will be based on a previous study of omega-3 fatty acids and their effects on up-regulating the TH1/TH2 ratio by ~32.5% [27]. The type I error is 0.05 and the power is 80%. Considering a dropout rate of 20%, we aim to recruit 120 subjects. The treatment group and the placebo group were assigned 60 participants each. Based on the grouping of our experiment, we will be divided into high exposure group and low exposure group according to PM2.5 exposure. In the high and low exposure groups, 30 subjects were treated with omega-3 fatty acids and placebo.
Selection criteria
Participants for this study will be recruited from long-term employees of the Chengdu subway system, who do not routinely wear professional anti-PM2.5 masks.
Inclusion criteria for the high PM2.5 exposure group include:
- Employees of the Chengdu subway system, regardless of gender, 20-65 years of age, who work in one of the station halls ≥3 times per week, ≥8 hours per day, and have been on the job continuously for ≥2 years;
- No obvious abnormalities detected by a physical examination in the past one year;
- Have not received hormones, antioxidant supplements (vitamin C, vitamin E) or non-steroidal anti-inflammatory drugs in the past three months;
- No history of surgery in the past three months;
- Willing and mentally competent to consent to participate in this experimental study and to sign an informed consent document.
Inclusion criteria for the low PM2.5 exposure group include:
- Employees of the Chengdu subway system who work in offices (with an air-conditioning device equipped with PM2.5 filters), regardless of gender, 20-65 years of age, who work in the office ≥3 times per week, ≥8 hours per day, and have been on the job continuously for ≥2 years;
- No obvious abnormalities detected by a physical examination in the past one year;
- Have not received hormones, antioxidant supplements (vitamin C, vitamin E), or non-steroidal anti-inflammatory drugs in the past three months;
- No history of surgery in the past three months;
- Willing and mentally competent to consent to participate in this experimental study and to sign an informed consent document.
Exclusion criteria
- A long-term history of drug use;
- Routine use of a PM2.5 respirator that complies with China's "PM2.5 Protective Masks" group standard (TAJ 1001-2015) during work;
- A history of smoking;
- A history of bleeding;
- An allergic reaction to flaxseed, fish and/or seafood;
- A history of hepatitis, fatty liver, cirrhosis, cholecystitis or gallstones;
- Currently pregnant or lactating;
- Participation in another clinical trial within the past six months;
- Inability to understand the intention of the experiment and inability to cooperate with the experimental procedure.
Randomization, allocation and concealment
Before the subjects agree to participate in this study, all qualified subjects who satisfy the inclusion and exclusion criteria will be given an information sheet describing the study and an opportunity to ask questions and clarify their concerns with the investigators. During the study, both the participants and the researchers will be blinded to the grouping information for each subject based on PM2.5 exposure level. BMISPSSStatistics24.0 software will generate 120 random numbers, and PM2.5 high-exposure group and PM2.5 low-exposure group will each allocate 60 random numbers. The researcher in charge of blinding will use two opaque envelopes to seal the random numbers, and will carefully check whether the serial numbers and drug numbers on the cover and letterhead are consistent with the labels on the drug packaging. Each subject will be provided with a corresponding emergency envelope. If the subject has a serious adverse event during the trial, the researcher will open the envelope after documenting the adverse event to break the blinding so that the subject can receive proper treatment.
Intervention
We plan to recruit 120 subjects who will be automatically divided into two groups based on their PM2.5 exposure level in the work environment: high PM2.5 exposure group (n=60) and low PM2.5 exposure group (n=60). In the high-exposure group, 30 people will receive omega-3 fatty acid treatment and the other 30 subjects will receive placebo treatment. Participants in the low-exposure group will receive an identical treatment regimen.
- Intervention group: Participants will receive treatment from the same batch of omega-3 fatty acids (1200 mg/capsule) provided by Kirkland, Canada. Participants will take two capsules every morning for eight weeks, and will be followed for 24 weeks after the trial. The omega-3 fatty acid capsules will be stored in a dry environment at room temperature.
- Placebo group: Participants will receive placebo treatment, containing soybean oil as the main ingredient, which has been produced by the Placebo Experimental Center of the School of Pharmacy, Chengdu University of Traditional Chinese Medicine. The physical appearance and weight of the placebo will be the same as the omega-3 fatty acid capsules, and the administration methods, experimental period and storage methods will be identical to those in the intervention group.
- The capsules for the intervention group and the placebo group will be packaged in the same box. Each box will contain eight weeks of drug dosage and will include the name of the subject, dosage, consumption schedule, description of storage conditions and expiration date. "Experiment only" will be highlighted in a prominent position on the box. We have selected soybean oil as the placebo (comparison) agent because it is commonly used in daily cooking, its physical properties are similar to omega-3 fatty acids and it has no obvious effects on TH1/TH2 polarization [28].
- The drug to be used in this project is a nutritional supplement with controllable safety risks. the participant may do so if he/she has no adverse events or side effects. However, if the subject has diarrhea or nausea, their participation in the trial may be suspended and the adverse event will be reported to the research team. Due to the special nature of omega-3 fatty acids, we will prohibit participants from using antioxidant supplements, such as vitamin E, during the trial. Medications used by participants to treat other diseases will not be curtailed or changed. If omega-3 fatty acids are beneficial to subjects with high PM2.5 exposure, we will put the control subjects on the "waiting list", that is, after the trial, the control subjects will also be provided with omega-3 fatty acids for 8 weeks free of charge.
Data and sample collection
We will use the Chinese Clinical Research Public Management Platform (Res Man) to collect and manage the data. The experimental data can only be accessed and manipulated by the research team.
The person in charge of the project will have access to the real-time data, but cannot make any changes to the data.
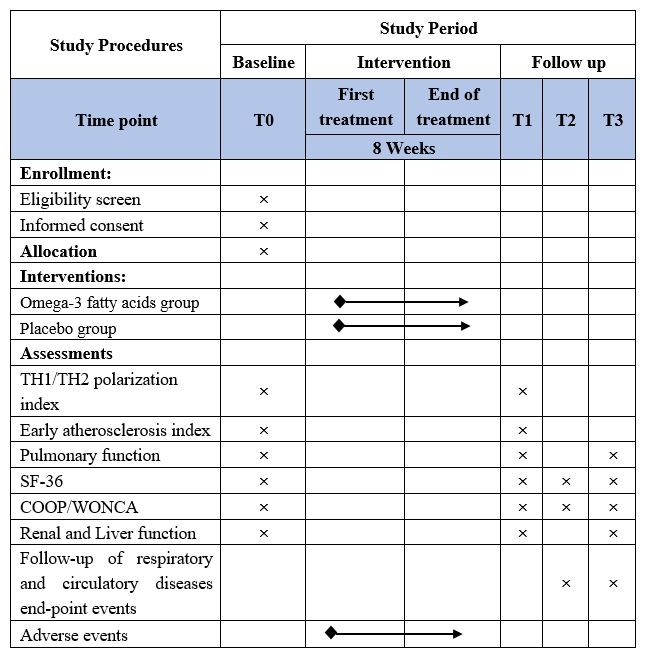
All data collectors will receive uniform training to ensure that data collected through questionnaires will have high quality and consistency. The Short Form Health Survey 36 (SF-36) [29], designed to assess quality of life through a comprehensive assessment of physical, mental and social components and COOP/WONCA charts will be completed at baseline, immediately after the final treatment(T1) and then at 12 weeks(T2)and 24 weeks(T3) after the final treatment. A pulmonologist will collect data on pulmonary function from all subjects to ensure consistency prior to and following the final treatment, as well as 24 weeks after the final treatment. We also will examine the follow-up records for each patient regarding respiratory and cardiovascular diseases at 12 weeks and 24 weeks following treatment. The time frame for data collection and assessments is shown in Table 1(the SPIRIT figure).
The number of TH1 and TH2 cells in the peripheral blood of subjects and the TH1/TH2 ratio will be measured at the time of enrollment (baseline) and again following treatment. Similarly, we will determine the TH1/TH2 polarization state, including the concentrations of serum interferon-γ (IFN-γ), interleukin-4 (IL-4), interleukin-12 (IL-12), interleukin-6 (IL-6), interleukin-8 (IL-8) and intercellular adhesion molecule-1 (ICAM-1), as well as liver and renal function to assess drug safety, at baseline and following treatment.
The concentrations of TH1 and TH2 cells in the peripheral blood immune cell population will be detected by flow cytometry using a CytoFLEX Flow Cytometer (Beckman Coulter, Brea, California, USA). Serum IFN-γ, IL-4, IL-12, IL-6, IL-8 and ICAM-1 levels will be measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits. Liver and renal function will be assessed in the Laboratory of Hospital of Chengdu University of Traditional Chinese Medicine. The blood products of all subjects will be destroyed uniformly after the end of the study.
Primary outcome measureOutcome measures
We will evaluate the concentrations of TH1 and TH2 cells in peripheral blood and the TH1/TH2 polarization state (IFN-γ, IL-4, IL-12 and IL-6) prior to and following treatment, and calculate the TH1/TH2 ratio using the IFN-γ/IL-4 balance index. We will examine differences in these indicators between the treatment and placebo groups.
Secondary outcome measures
- A pulmonary function test will be performed to evaluate the impact of PM2.5 on lung function in each subject.
- Early indicators of atherosclerosis, including IL-8 and ICAM-1, will be measured.
- The SF-36 questionnaire will be used to assess the health status of each subject and to generate a COOP/WONCA chart. The quality of life will be summarized for eight aspects: physical functioning, physical role functioning, physical pain, general health, vitality, social functioning, emotional health and mental health.
- Safety and adverse reactions to drug treatment will be monitored.
Adverse events’ reporting and safety monitoring
The omega-3 fatty acids used in the project are a nutritional supplement with controllable safety risks. The Chinese Ethics Committee of Registering Clinical Trials (Ethical Review No.: ChiECRCT20190343) has approved this study. If the subject has any adverse events related to this study (such as diarrhea or nausea), it will be reported to the research team and recorded in the CRF. The project supervisor will also collect adverse events in a timely manner and decide on follow-up treatment (including close observation, additional medical management, or early termination).
Data management and monitoring
Data collection and monitoring will be managed by a dedicated Data and Security Monitoring Board (DSMB). The DSMB will be composed of a deputy chief physician from the respiratory department, a junior Chinese medicine practitioner and a statistician. DSMB members will provide appropriate recommendations on the safety and completeness of all procedures during the clinical trial. All completed questionnaires and laboratory results will be stored in a locked cabinet. The data will only be accessible to the researchers. Two data entry clerks will enter all data into an electronic database at the same time. The electronic database will be maintained as a password-protected file.
Statistical methods
IBM SPSS Statistics V.25 software will be used for statistical analysis of the data collected in this study. Subjects who withdrew from the experiment but received at least one treatment will still be included in the intention-to-treat analysis. We will use various attribution methods to conduct sensitivity analysis to test whether the results are reliable for different assumptions about missing data. Demographic and baseline data will be tabulated and evaluated using analysis of variance (ANOVA) or the χ2 test. Analysis of variance was performed on categorical variables, and Pearson χ2 test was performed on continuous variables. 95% CI will be used for continuous variables. In this study, all statistical tests will be two-way, and P value <0.05 is considered valid.