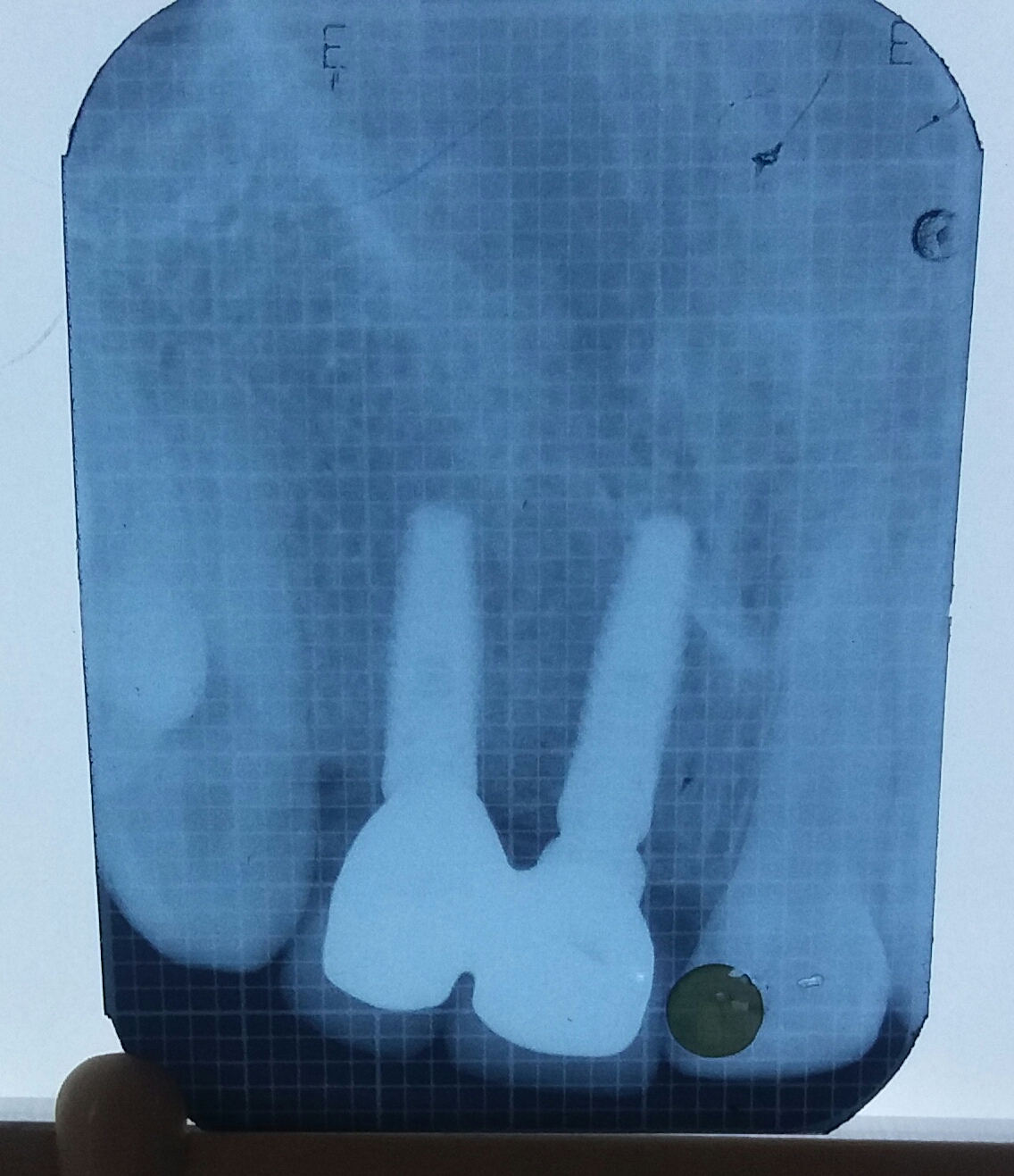
Healthy osseous contour provides a skeleton for peri-implant soft tissues. The purpose of atraumatic extraction is to minimize bone resorption and to maintain alveolar ridge dimensions during healing. In present study, socket preservation was done by using a combination of PRF, β-TCP and rh-BMP-2.After 3 months of ridge preservation clinical examination of the ridge revealed minimal dimensional changes ( mesio-distal bone loss 0.6 ± 0.13 mm and bucco-lingual bone loss 0.5 ± 1.13 mm).The clinical hardness of bone evaluated during drilling, prior to implant placement, provided a tactile sensation analogous to drilling into spruce or white pine wood at all the four sites.(13) Although the density of bone could not be evaluated using Hounsfield units, dense to thick porous cortical bone on the crest and coarse trabecular bone underneath was seen on radiographic examination, suggesting D2 bone quality(14). Histologically, presence of vital, mineralized osteoid trabeculae along with soft tissue containing spindle nuclear cells indicating new bone formation was noted. All four implants achieved good primary stability.
As soft tissue grows six times faster than the bone tissue (15), in the present study the sockets were covered with a saddle of PRF membrane which prevented the gingival connective tissue down-growth. It prevented epithelial migration into the defect. It also held osseous graft in place. (16) Additionally, the membrane also aided in clot stabilization. PRF principally contain fibrin matrix rich in platelets, leukocytes. Cytokines such as IL-1𝛽, -4, and − 6, and growth factors such as PDGF, TGF-beta, IGF, EGF and VEGF are other important components. These are the key elements in bone regeneration. (17) Fibrin gels in coagulation cascade aids in fibrinogen molecules collaboration. This leads to a highly biocompatible three-dimensional fiber network. (18)Therefore, PRF resulted in improved wound healing and enhanced bone graft density and maturation. (19)
β -TCP is (purified, microcrystalline porous) form of calcium phosphate. A remarkable resorption of β -TCP particulate is estimated around 3 to 6 months after placement. Besides, particles become well-incorporated into new bone formation. This creates a dense cancellous matrix. Biodegradation of graft takes place by osteoclastic activity as well as chemical dissolution by tissue fluids. During implant placement, a solid new bone formation was evident which favored the placement of an ideal implant size.
The use of rhBMP-2 necessitates the use of a carrier for its oseoinductivity (20) Misch emphasized advantages of rhBMP-2 in new bone growth in patients requiring extraction. In present case series rhBMP-2 was used as an agent to promote socket repair as well to aid in ridge augmentation when combined with a part of β -TCP. Fiorellini et al (21) determined the efficacy of varying concentrations of rhBMP-2 in socket defects. The results showed profound bone growth when rhBMP-2 concentration was increased. Author also stated an ideal concentration for rhBMP-2 in grafting could be 1.5 mg/mL. Therefore, in the present study 1.5 mg/mL concentration of rhBMP-2 was used.
Various studies (22) (23)have supported the use of a mixture of β-TCP and rh-BMP- 2 to facilitate increased bone formation in the defects. Therefore, in this study rhBMP-2 was used in combination with β-TCP to promote bone growth.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}