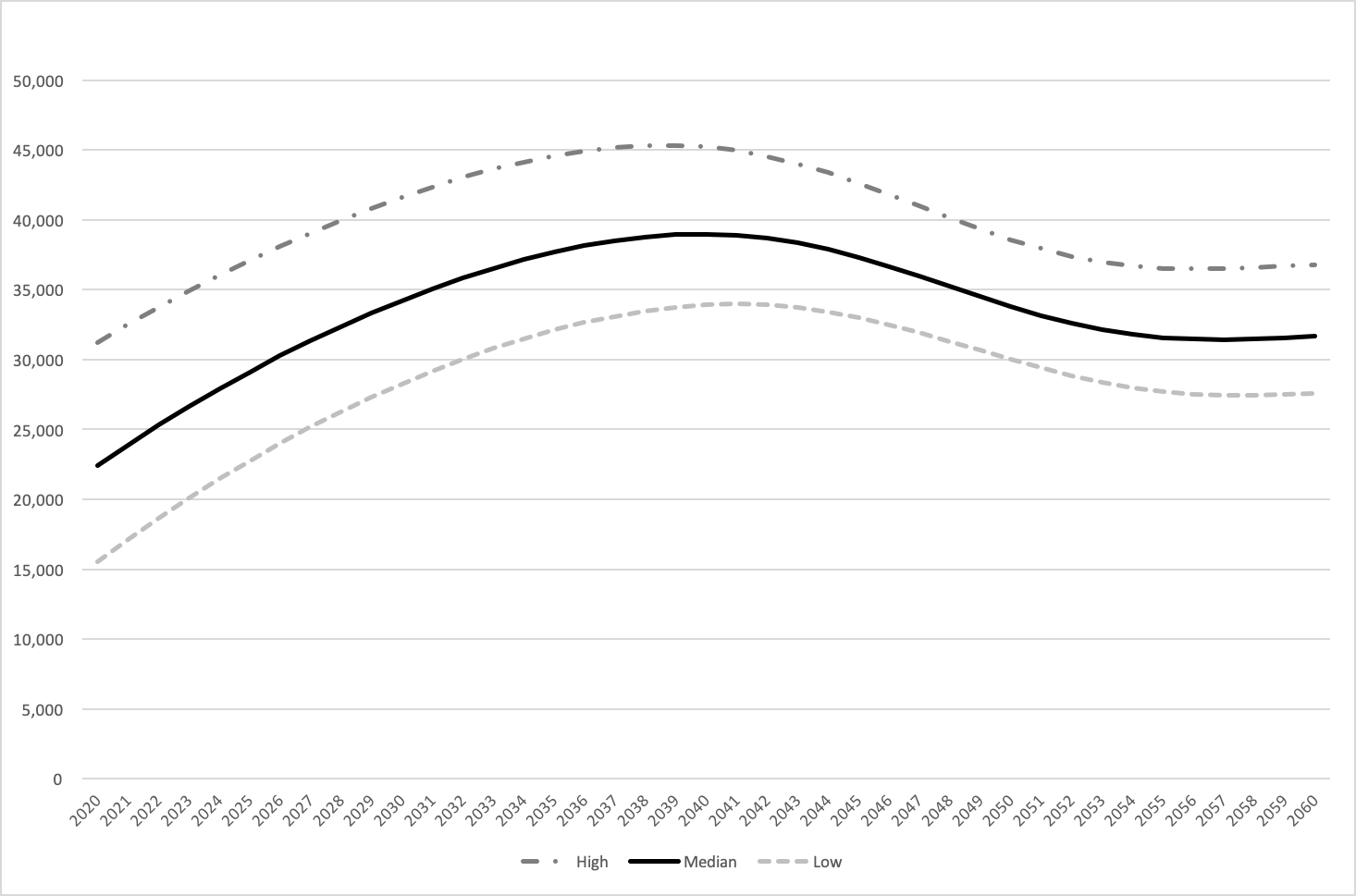
We found that Japan will need an additional 22,000, or 1.59 times the current number of home care physicians by the mid 2030’s. However, our study also shows that developing home care may help suppress the growing overall need for physicians. Further, demand for home care physicians will diminish after 2040.
Based on our projections, demand for home care physicians will have at least doubled by 2040. The estimation of future hospital deaths was based on three assumptions: the pragmatic and dynamic government models, and the non-intervention model. Among these, the non-intervention model is unrealistic considering dropping hospital admission statistics including total hospitals, total beds, and average stay length [23]. The dynamic government model (about 54,000—125,000 physicians in 2040) might underestimate the number of hospital deaths because of the steadily increasing aged population despite the whole population shrinking and the present and future longest life expectancy in the world until the year 2100, which implies a constant need for hospital beds [1]. Considering this, we believe that the pragmatic model (about 46,000—100,000 physicians in 2040) is the most realistic projection. Hence, in order to supply sufficient home health care smoothly preparing for growing aged population, our results suggest that the Japanese government must increase the number of skilled home care physicians. However, the results also suggest that demand for home care physicians will decrease long-term. Therefore, reduction in home care physician training should be considered in the 2030’s.
Our analysis employed two methods: the health and service needs method, and the workforce-to-population ratio method. In the first, we used mortality among home care patients in the previous multi-center study with a sufficiently narrow 95% confidence interval. We regarded this as a modification of the health and service needs approach which, though simple, supplies reliable projections by considering the influence of multiple factors such as political action and patient needs for home care physicians. Second, the physician-to-patient ratio method, which is a variant of the workforce-to-population method, is straightforward and widely used [24]. Although it has some potential drawbacks such as future homogeneity of the physician-to-patient ratio, we used it in a supplemental capacity, and it produced similar results.
While our methods depend on some assumptions, our estimations are highly reliable. This is evidenced by the small difference between our mortality method mid-estimation and the present number of home care physicians in 2017, which are reached through wholly different methods. Where the mortality method is based on the number of future home deaths and mortality, the present number of home care physicians is based on counts of clinics and hospitals and physicians per institution. Furthermore, our results agree with past studies forecasting numbers of physicians, which anticipated increases into the 2030’s [25, 26]. We are therefore convinced that our projections are not unreasonable.
While many medical workforce analyses have covered physicians, primary care physicians, surgeons, specialists, and nurses, we are aware of no published reports projecting home care physicians at the time of this writing. The problems of an ageing society are not peculiar to Japan and industrialized countries; the elderly population in developing regions is increasing more rapidly than in developed regions [2]. Much might be learned from Japan’s response to these issues. This study employed relatively simple methods with potential for broad application: the health and service needs approach and the workforce-to-population ratio approach [11].
There are some limitations to our study. First, our estimations were limited by the accuracy of available data, including the fact that the future nursing home death number was based on patient preferences [18]. Also, our mortality data comes from an interim analysis presented at an annual conference, although we believe the figures are precise [19]. Second, while our two methods produced similar projections, which suggests valid estimations, it is difficult to completely account for present and future variability, such as drastic changes in health policy or natural calamities. Our results depend on the average yearly number of home care patients per physician, which can vary over time and according to public policy. Geographical disparities and other variables such as future development of nurse practitioners affect the number of physicians, with wide gaps between physician-rich and physician-poor areas [27]. Finally, practical constraints required us to make several assumptions in applying the available data. For example, we applied the physician-to-patient ratio from home deaths in 2014 to future home and nursing home deaths. With accurate nursing home physician data, we could estimate more precisely. Further, while the mortality approach mainly focuses on home care support clinics, the physician-to-patient ratio approach includes home care support and ordinary clinics. All of these limitations should factor into further studies projecting numbers of home care physicians.
{kind=link}
{kind=link}