Our approach successfully achieved unilateral, joint-specific restrictions in range of motion (ROM) in an isolated fashion at the ankle, knee, and ankle+knee simultaneously. This framework allowed us to separate the relative impact of ankle versus knee restriction and understand their interaction on mechanical compensations and the resultant energetic penalties during walking. This research builds upon previous studies in which the ankle [37] or knee [19] were braced independently. These results can help optimize future designs of rehabilitative techniques and technology by providing insight into trade-offs of intervening at one lower-limb joint versus another.
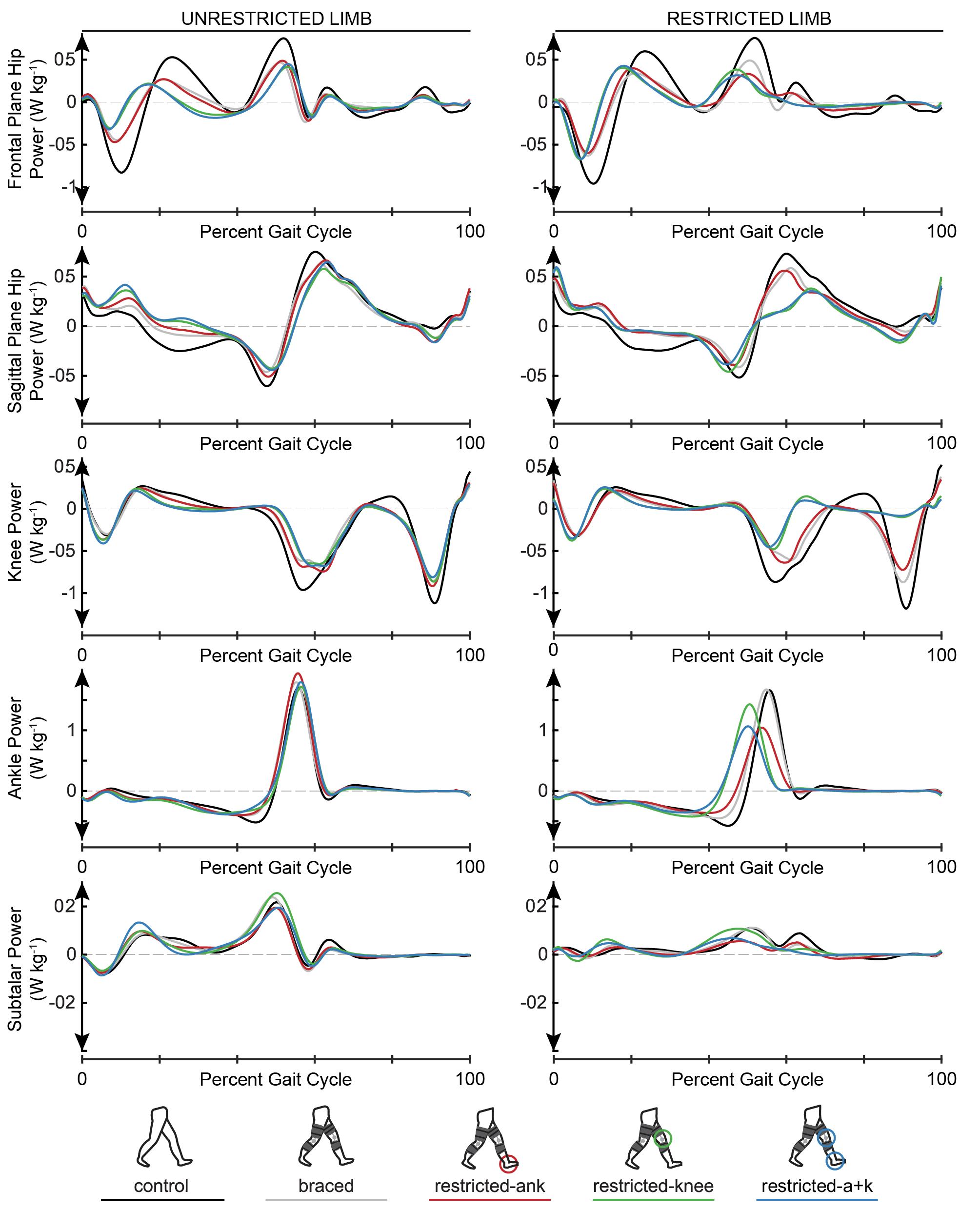
In support of our first hypothesis, the use of our custom 3D-printed ankle stay produced a reduction in ankle ROM, which in turn attenuated peak ankle power at pushoff (Figure 1 A,C) and reduced peak restricted limb propulsion (Figure 2A). Specifically, when the ankle was restricted, with or without locking the knee, we observed reductions in both peak ankle power and peak limb propulsion. In contrast, locking the knee did not lead to a reduction in peak propulsion (Figure 2A), providing further evidence that ankle impairments alone may be responsible for commonly observed propulsive deficits in pathologic gait.
We hypothesized that reductions in propulsion resulting from limited ankle mobility would necessitate sagittal plane compensations at both hips; however, Dsagittal plane average positive hip power only increased on the restricted limb when comparing the restricted ankle condition to the restricted knee and combined ankle+knee conditions (Figure 3 A,B). DSagittal plane average positive hip power did not increase whenever the knee was locked, suggesting that the additional restriction at the knee prevented a sagittal plane hip compensation. It is possible that the restriction at the knee made foot clearance a priority or limited the hip flexor’s capacity to initiate passive knee flexion, thereby reducing motivation for in-plane compensation.
With respect to our second hypothesis, the restriction of knee ROM, with or without the ankle restriction, contributed to an increase in circumduction when compared to only locking the ankle (Figure 2B). Interestingly, the increases in circumduction observed in knee-restricted conditions were not significantly larger than the braced condition, and the circumduction values found in the braced condition were larger than values reported with the ankle locked, although not significantly. We cannot attribute this finding to wearing unrestricted knee braces because knee braces were worn in all conditions except the control. It is possible that bracing the ankle and the resulting increases in sagittal plane hip power limited hip motion in the frontal plane.
We must reject part of our second hypothesis, as we did not observe the increases in frontal plane hip power that we hypothesized would facilitate circumduction of the foot (Figure 3B). Instead, we found that participants opted to hip hike (i.e., decrease pelvic list) during restricted limb swing to enable circumduction when the knee was restricted (Figure 3C). Interestingly, all restricted conditions had negative Dhip power in the frontal plane, indicating that any bracing reduced hip power generation when compared to the braced condition (Figure 3B). This finding contrasts with the previously observed increases in frontal plane non-paretic hip power reported for persons-post stroke [12]. It is possible that the isolated bracing in our study left pelvic list as the simplest compensation for our participants, whereas individuals post-stroke typically are contending with alterations in motor control and activation in addition to stroke-induced weakness.
Our approach of restricting motion at a joint mimicked many gait characteristics of post-stroke walking (Figure S1-4). Locking the ankle resulted in reductions in ankle ROM comparable to paretic ankle ROM values reported in literature [26]. Reductions in knee joint velocity at pushoff induced by knee restriction were within the range of velocity values reported in stiff-knee literature [52]. The peak ankle powers were within the range of values seen previously in stroke survivors walking at similar speeds [26]. Propulsive symmetry decreased in all of the restricted conditions when compared to the unrestricted condition and peak restricted limb propulsion values for conditions with restricted ankle motion were within, [24, 53] but generally on the higher end of values seen in post-stroke literature [17, 53, 54]. When the knee was locked, we observed increases in circumduction and decreases in peak knee flexion that were very similar to values reported in the literature for persons post-stroke [16, 18, 40, 49, 52, 55].
Despite our success in inducing gait characteristics common to post-stroke, our metabolic results did not support our third hypothesis that restricting the ankle would be more expensive than restricting the knee joint (Figure 4B). Nevertheless, our results suggested an energetic impact due to ankle restriction. Specifically, our data indicated that combined restriction of the ankle and knee was more metabolically detrimental (i.e., larger positive Dmetabolic cost) than restriction of just the knee. Furthermore, all conditions that restricted the ankle (i.e., restricted-ankle and restricted-a+k) were more metabolically costly than the braced condition, suggesting that regardless of restrictions in knee ROM, any direct restriction on the ankle was metabolically detrimental. These results provide support for the potential of ankle-based rehabilitative techniques or technologies in persons post-stroke or other lower extremity joint deficits to provide a metabolic benefit [26, 56-59].
We anticipated that the increases in metabolic cost during the restricted conditions would be attributed to altered joint power requirements, consistent with findings from post-stroke gait [12, 13, 60, 61]. In particular, we expected that greater metabolic cost would be due to a combination of the concurrent transfer of power from more to less efficient joints, thereby requiring more metabolic energy to achieve the same mechanical power output and increased total average positive joint power [19, 37]. Specifically, we anticipated a bilateral increase in hip power would accompany an ankle restriction, indicating that joint power requirements were transferred from the highly efficient ankle to the less efficient hips. Instead, we only observed an increase in average positive hip power for the restricted limb in the restricted-ank condition when compared to the braced condition (Figure 3A). Further, an increase in total positive joint powers does not appear to explain the increased energetic requirements because whereas metabolic cost tended to increase across all restricted conditions (Figure 4), the average positive joint power tended to decrease compared to the unrestricted condition (Figure 5). This contradicts prior work on mechanics and energetics of walking in persons post-stroke which has suggested that increases in net metabolic power are accompanied by increases in total average positive joint power without a change in the efficiency of positive mechanical work [12, 13, 60, 61]. While a decrease in total average positive joint powers between conditions with equivalent walking speed may seem counterintuitive, an increase in gait cycle duration would allow for the conservation of total joint work. Additionally, we did not observe a significant correlation between Dtotal average positive joint power and Dnet metabolic power (Figure 6). Overall, changes in total average positive joint power were a poor indicator of changes in net metabolic power study-wide (Figure 4-6, Fig S5). Thus, in general, it need not be true that changes in metabolic cost are driven by changes in positive mechanical power under conditions with restricted joint ROM. It is possible that this discrepancy in findings is due to the inherent differences in mechanically-induced joint restrictions used here and the unilateral muscle weakness and altered muscle control present after stroke. Specifically, while our study was able to reproduce ‘stroke-like’ gait by restricting joint kinematics, we do not reproduce neural changes altering muscle-level coordination complexity [36], changes in muscle reflex coupling [62], or changes in muscular contraction efficiency [6] that exist post-stroke. These results warn that the use of positive joint power as a proxy for metabolic demand when analyzing atypical walking may be tenuous [63]. Other factors, such as muscle activation and effort, may be more relevant to mechanisms driving metabolic cost [64, 65].
There are limitations to this work that require consideration. While bracing at the ankle and knee restricted ankle excursion and knee velocity to values within the range reported for persons post-stroke, we cannot account for the neuromechanical changes that accompany a stroke (see above). We recognize that participants may have used the trunk and upper extremity to compensate for restricted lower limb motion, and the way in which the upper limb was used may also affect the lower limb mechanics reported here. If we had these data, our regression analysis of total average joint powers may be a stronger predictor of metabolic cost. As we look to generalize these results to impaired populations it is important to note that neurological injury could restrict upper limb compensations and have possible effects on measured lower limb function. Additionally, as part of a larger study examining bilateral vs. unilateral restriction, our participants’ knee braces were worn bilaterally (albeit unrestricted on one side in all conditions) and may have altered gait when compared to the unbraced control. We attempted to account for this limitation by comparing the restricted conditions to the braced condition, during which the knee braces were both worn unrestricted. Our choice to compare to the braced condition was made to eliminate the impact of the additional mass of the knee braces. An ankle stay was added onto the participant before the restricted-ank and restricted-a+k conditions and removed following the conditions so it is also possible that the added mass of the ankle stay could have impacted outcomes; however, the ankle stay was 3D printed out of PLA and weighed less than 3 ounces, and therefore we do not believe the risk of mass-related impacts to be significant. While the exact amount of time needed to acclimate to unilateral bracing is unclear, we attempted to mitigate this limitation by analyzing walking trials from the last two minutes of each seven minute condition. The participants of this study were on average significantly younger than the average person post-stroke, which may impact generalizing our results to older populations. Comfortable overground walking speed in persons post-stroke can also be significantly less than 0.8 m s-1, the speed participants walked in this research. However, the walking speed chosen here was designed to be fast enough to challenge the walkers and elicit metabolic changes, but slow enough for them to complete the braced trials. Lastly, we cannot generalize our results to a situation where existing joint or limb limitations led participants to reduce walking speed; future research could investigate the impact of joint restriction on gait compensations and metabolic consequences across walking speeds.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}