Nepal with a population of about 27 million, has been ranked with the highest level of maternal mortality (1). Between 1996 and 2016, the maternal mortality ratio has reduced from 539 to 239 per 100,000 live births (1) (2). However, this reduction ratio is slow. In Nepal, various groups have diverse cultural beliefs concerning pregnancy and delivery care (3). In many communities, being pregnant is taken culturally as a subject of fate. (4). However, in fact, maternal health refers to the health of women during pregnancy, childbirth, and the post-natal period, that encompasses the health care dimensions of family planning, preconception, prenatal and postnatal care in order to reduce maternal mortality and morbidity (5). Similarly, maternal death or maternal mortality is defined by World Health Organization (WHO) as "the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any causes related to or aggravated by the pregnancy or its management but not from accidental or incidental causes" (6).
Chiefly, maternal death takes place in developing countries rather than in developed countries. Nepal, like other countries in South Asia, has long been overburdened with maternal health problems (6). According to Nepal Maternal Morbidity and Mortality Survey (NMMMS) 2008/09, 41% of maternal deaths take place at health institutions, 40% at home, and 14% on the way to health facilities (2) (1). The NMMMS survey also reported that in Nepal 69% of maternal deaths were due to direct causes that include hemorrhage, then eclampsia, abortion-related complications, gastroenteritis, and anemia while 31% were due to indirect causes (7) (8).
As per WHO postpartum hemorrhage, unsafe abortion, infection, preeclampsia, and long obstructive labor are the major causes of maternal death in Nepal. (7).
An important measure to minimize maternal mortality is to make quality maternal health services affordable, accessible, and increase the timely utilization of those services.
Nepal has set a target of 70 percent to achieve all deliveries by SBAs and at institutions by 2020 in order to achieve the SDG target in 2030. Safe motherhood is one of the prioritized program in Nepal and thus promoting safe motherhood through different initiatives such as the provision of the aama and newborn program. Under this program, every woman immediately after institutional delivery gets a cash payment of NPR 3,000 in mountains, NPR 2,000 in hills, and NPR 1,000 in Terai districts as transportation incentives. As 4 ANC incentives, women get NPR 800 on completion of four ANC visits at 4, 6, 8, and 9 months of pregnancy. Institutional delivery and postnatal care services are freely available through birthing centers and hospitals. Further, under the nyano jhola program, every woman who gives birth at health facilities gets two sets of clothes (bhoto, daura, napkin, and cap) for newborns and mothers, and one set of the wrapper, mat for baby, and gown for mother. The provision is made to protect newborns from hypothermia and infections and to improve the utilization of birthing centers located at the local level. Moreover, subsidies are also provided to health facilities for free delivery care based on deliveries conducted (8).
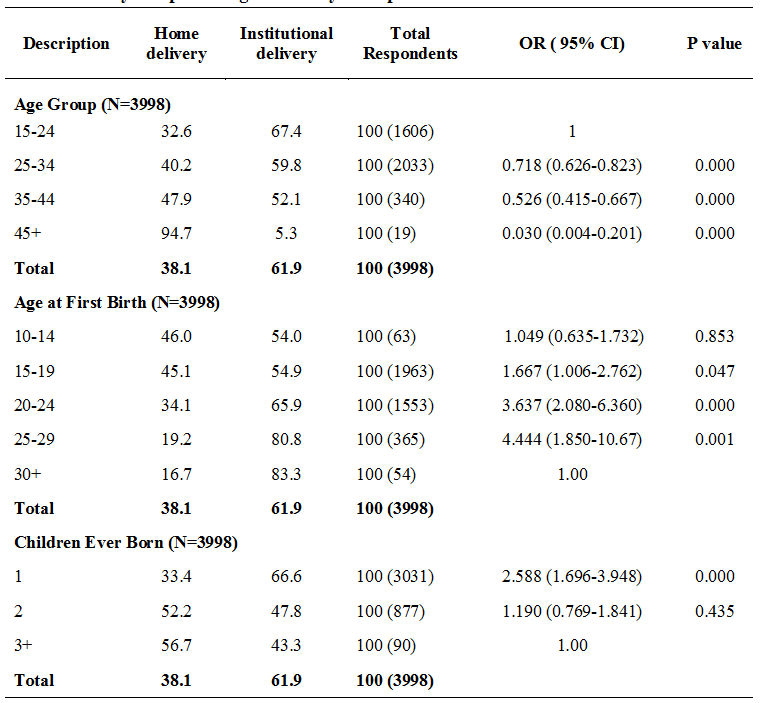
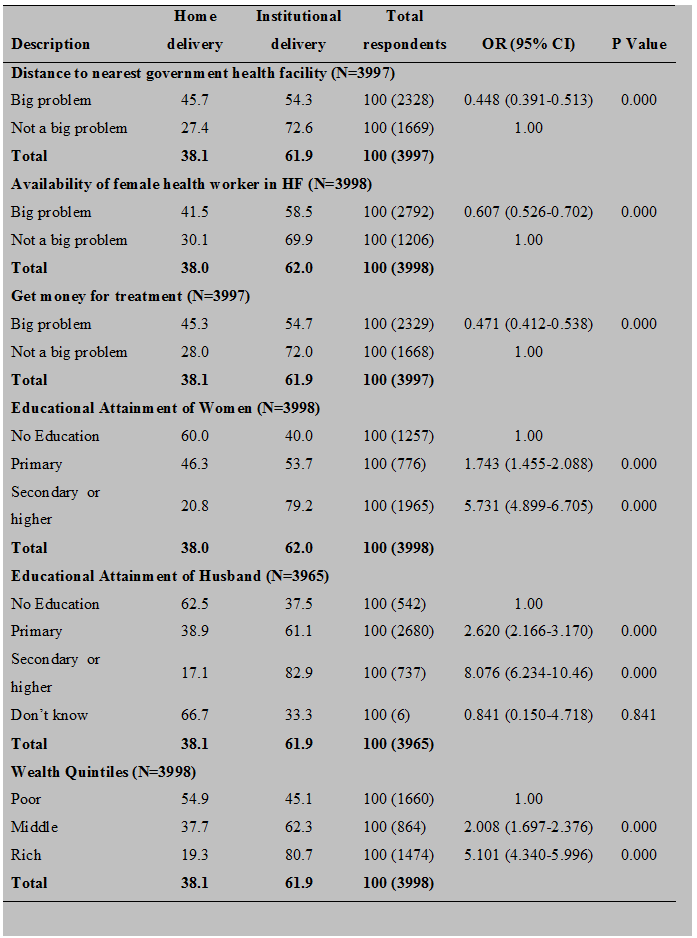
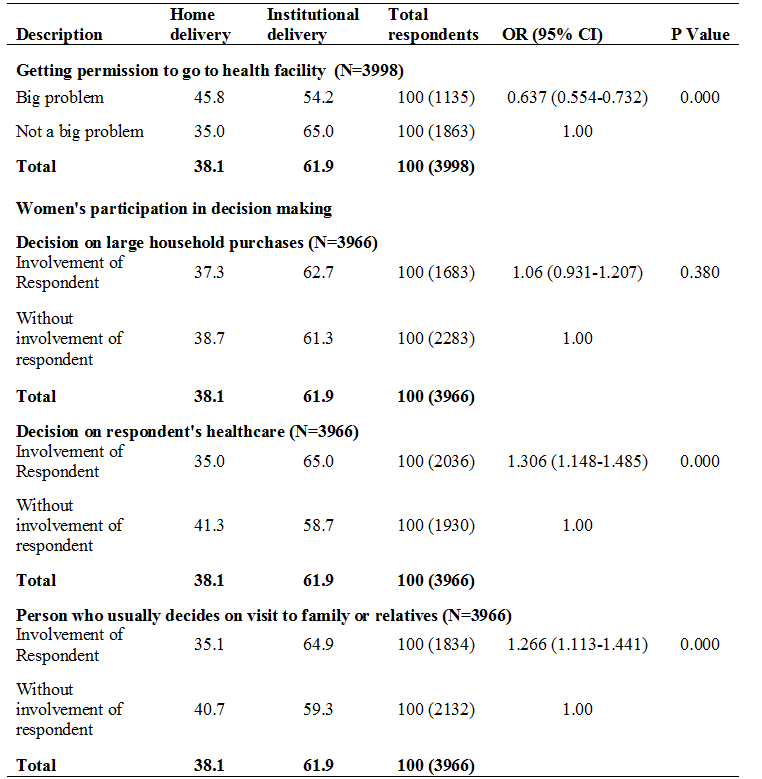
The literature on factors affecting place of delivery showed the effects of various demographic, socio-economic, and empowerment factors either women deliver in an institution or at home. The studies have revealed that various demographic, socio-economic and empowerment factors play an important role to determine the place of delivery in Nepal. Particularly in Nepal, women's age, caste, ethnicity, parity, education of mother and spouse, occupation, household income, time to reach the nearest health facility, decision-making powers, and harmful cultural practices & traditions are the major factors affecting the usage of institutional delivery. (9) (10) (11) (12).
Against this background, this paper aims to answer the research question: What are the demographic, socio-economic, and empowerment factors among women that could affect the place of delivery in Nepal?
The Nepal Demographic Health Survey presents information about the place of delivery only on status, trends, and patterns by background information. Whereas further analysis of NDHS reports analyzed data set of women who met both criteria i.e had a live birth in the 5 years preceding the survey and experienced domestic violence. However, this paper presents rigorous analysis derived from cross-tabulation and logistic regression examining the effect of various demographic, socio-economic, and empowerment factors on the place of delivery. The findings of this study might be helpful for program planners and policy in order to generate policy and design specific maternal health programs aiming at different provinces, rural communities, and different social groups in Nepal.