Research subjects and grouping
A total of 1536 patients, who received PELD in our hospital from January 2015 to June 2019. Fifty patients who suffered from PELD recurrence and underwent reoperation (PELD or MIS-TLIF surgery) were enrolled in the study, and the retrospective analysis was performed. Before operation, surgeon presented a detailed written informed consent to the patients. This study was approved by the Human Subjects Institutional Review Board at Peking University First Hospital. Patient outcomes were collected independently from participants with informed written consent, and data were analyzed blindly.
The inclusion criteria were as follows: patients who (1) underwent a successful PELD surgery which could be confirmed by a pain-free interval of at least 1 month, (2) recurrent pain symptoms and a magnetic resonance imaging (MRI) confirmation of a herniated fragment on the same level as the previous PELD surgery was achieved, and (3) conservative therapy failed to relieve the recurrent pain.
Exclusion criteria were as follows: patients who (1) the recurrent pain symptoms and MRI confirmation of residual disc fragment occurring within 1 month after the PELD surgery, which is defined as surgical failure, and (2) the herniated disc fragment did not appear at the same level as that in the previous PELD surgery.
In consideration of that the scar formation exists in patients receiving reoperation, to exclude scar formation from real rLDH, all the enrolled patients should exhibit the following characteristics: (1) definite neurological symptom; (2) space-occupying lesions in lumbar spinal canal that were confirmed by MRI; (3) the herniation of nucleus pulposus were observed intraoperatively. Also, the patients with vertebral instability or spondylolisthesis who preferred MIS-TLIF were excluded[14].
Based on these inclusion and exclusion criteria, 46 cases of 50 patients were involved in the following retrospective analysis, each of included patients was appropriate for each of these 2 surgical methods. The 46 patients were divided into the following two groups: PELD group (n=24) and MIS-TLIF group (n=22). Patients were fully informed of the details regarding these two surgical methods, including the surgical procedures, experience of the surgeons, complications and recurrence, total cost, and the final choices were made by the patients.
Surgical technique and postoperative management
Surgeries of patients in the two groups were performed by the same experienced surgeon.
PELD group: PELD was performed as described by Hoogland et al.[30] and H. Michael Mayer and Mario Brock[4]. The procedure was performed under local anesthesia with patients in the prone position on a radiolucent table. The patients were informed of all the procedure steps before beginning the procedure. The patients communicated with the surgeon throughout the entire procedure. After infiltration of the entry point (8-12 cm from the midline) with local anesthetics, an 18-gauge spinal needle was introduced under fluoroscopic guidance. The final target point of the spinal needle was the medial pedicular line on the anteroposterior image and the posterior vertebral line on the lateral image. The subsequent steps were as follows: (1) a guide wire was inserted through the spinal needle; (2) the spinal needle was removed; (3) a small skin incision was created at the entry point; (4) a tapered cannulated obturator was inserted along the guide wire; (5) after contacting the annulus, the obturator was inserted into the disc with hammering, and the timing of foraminoplasty was selected based on the type of prolapse of the disc; and (6) a bevel-ended, oval-shaped working cannula was inserted into the disc along the obturator. The obturator was removed, and an endoscope was inserted through the cannula. The herniated disc was removed using small forceps. A targeted fragmentectomy was performed in all cases. After the herniated fragment was completely removed, the endoscope was also removed, and a sterile dressing was applied with a 1-point suture (Fig. 1).
MIS-TLIF group: MIS-TLIF was performed as described by Foley et al [19]. All the participants received general anesthesia before MIS-TLIF surgery. C-arm machine and Quadrant System were prepared before the operation. The patient was placed in a prone position on a radiolucent operating table. Under C-arm fluoroscopy, the targeted level was confirmed according to our self-made locator. Based on the spatial relationship, the intervertebral spaces and the pedicle positions were marked on the body surface. An incision was planned by connecting a line between the outer portions of both ends pedicles (approximately 3.0 cm off midline). Then a skin incision about 2.0 to 3.0 cm was made on the more symptomatic side or more severe pathology side according to the imaging. The paravertebral muscles were split and retracted laterally to the outer edge of the facet joint, and the zygapophysis was confirmed. Expansion tube was then inserted and Quadrant System was placed. X-ray examination was repeated to confirm the target segments and the placement of Quadrant System. We conducted the decompression by cutting the inferior portion of the lamina, hypertrophied superior and inferior articular processes, and ligamenta flava. Then we enlarged the intervertebral space and appropriate bullet-type interbody cage (Medtronic Sofamor Danek, Memphis, TN 38132, USA) filled with autologous bone was packed into the center of intervertebral space. Following these, Ipsilateral percutaneous pedicle screws (Medtronic Sofamor Danek, Memphis, TN 38132, USA) were inserted through the same skin incision, and contralateral percutaneous pedicle screw was also placed through mirror incision under fluoroscopic guidance, also titanium rods (Medtronic Sofamor Danek, Memphis, TN 38132, USA) were inserted and tightened on both sides (Fig. 2). Finally, hemostasis and proper irrigation of the incision was performed and negative pressure drainage was placed followed by closure in layers.
For all the patients in the two groups, off-bed activities could be performed on the second day after the surgery under the protection of waist support. The drain removal was conducted when the drainage fluid for 24h was less than 30 ml[23] in MIS-TLIF group. The patients could return to non-manual work or school 2 weeks postoperatively and they were allowed to perform full activity 3 months after the surgery. We encourage sufficient bed-rest and off-bed activities under the protection of waist support within 3 months after surgery.
Clinical assessment
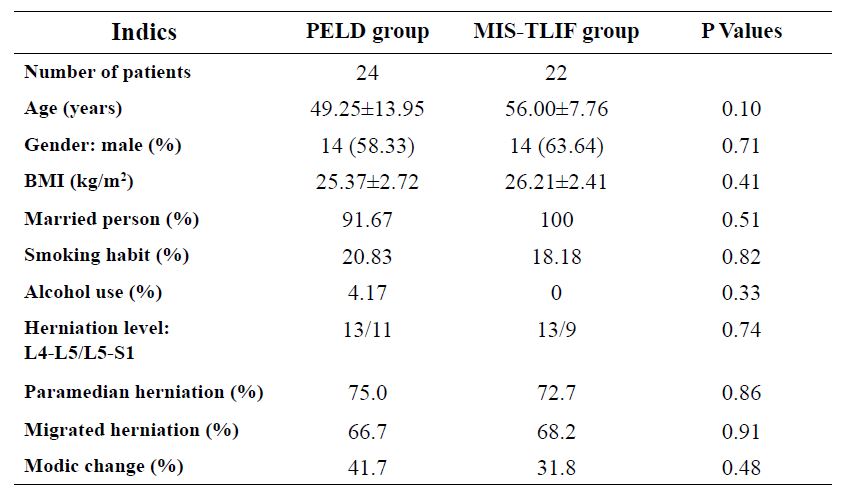
The preoperative data from all the enrolled patients were assessed in terms of demographic data (age, gender, body mass index [BMI], marital status, alcohol use history, and smoking history) and clinical data (herniation level, paramedian/central herniation, migrated/nonmigrated herniation, and Modic change).
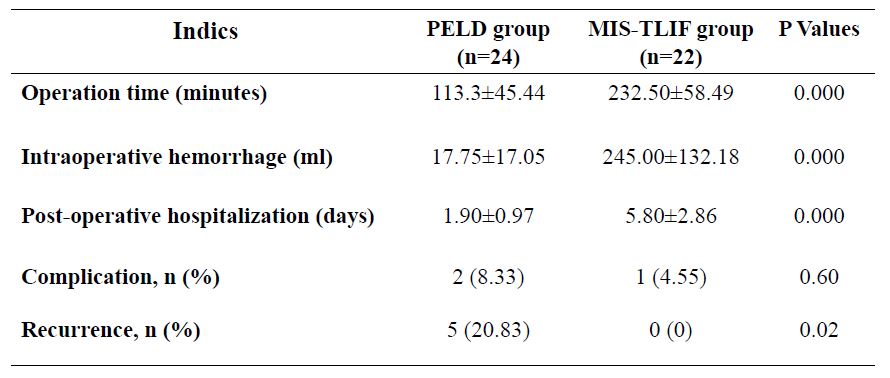
The perioperative conditions (operation time, intraoperative hemorrhage, and postoperative hospitalization), complications, and recurrence condition also were collected and evaluated.
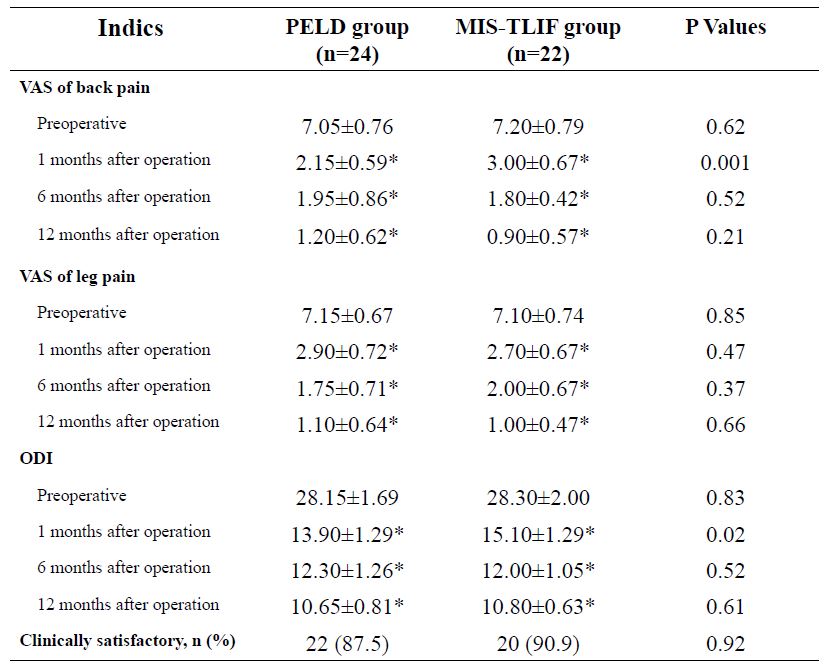
Clinical outcomes were analyzed based on the improvement of back and leg pain, disability, and clinically satisfactory rate. The intensity of back and leg pain were evaluated using visual analog scores (VAS) preoperatively and 1 months, 6 months, 12 months postoperatively. Disability was assessed using the Oswestry disability index (ODI) version 2.0 preoperatively and 1 months, 6 months, 12 months after surgery. The clinically satisfactory was assessed 12 months postoperatively by an independent surgeon using the MacNab criteria[31]. It was defined that excellent outcome as there is no pain and no limitation of normal life; good outcome as there is occasional pain or paresthesia, but no need medication, and no limitation of normal life; fair outcome as pain is somewhat improved but needs medication, and some limitation of normal life; poor outcome as no improvement or worsening, additional operation is needed due to incomplete decompression, development of instability. Excellent and good outcomes were rated as clinically satisfactory.
Statistical Analysis
Data were analyzed by Statistical package for program (Version12, SPSS, Chicago, IL). The statistic was demonstrated as mean ± SD. Independent student 𝑡-test was used to compare the difference of continuous variables between the two groups. Chi-square test was used to compare the difference of dichotomous variables between the two groups. These two tests were used to compare the baseline data and observation parameters between the 2 groups. 𝑃 < 0.05 was regarded as statistical significance.
 BMI: body mass index; PELD: percutaneous endoscopic lumbar discectomy; MIS-TLIF: minimally invasive transforaminal lumbar interbody fusion.
BMI: body mass index; PELD: percutaneous endoscopic lumbar discectomy; MIS-TLIF: minimally invasive transforaminal lumbar interbody fusion.