Study 2: Methods
Stimuli and procedure.
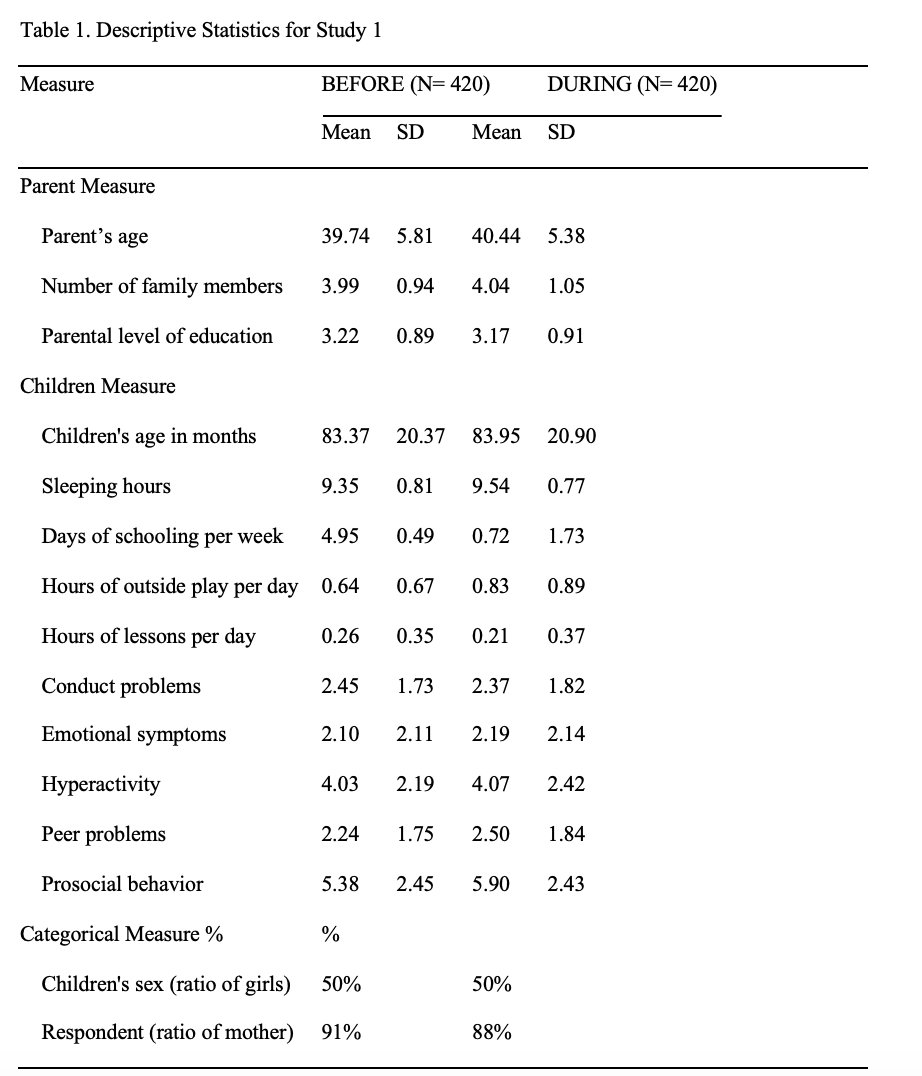
In addition to the background information in Study 1, parents were asked to complete the questionnaire about their own, and the children’s media use and skills for operating digital devices.
Media use. Parents responded to questions about their own, and the children’s media use. The questions were based on previous surveys of children’s media use in Japan (29). First, parents completed questions about the children’s media use. Specifically, parents reported the frequency of the media use per week (e.g., how often does your child use (MEDIA NAME) per week?) and per day (e.g., how many hours does your child use (MEDIA NAME) per day?). Media included TV, video, tablet computer, smartphone, non-portable computer, and non-portable games. Thereafter, parents also completed the questions about their own media use, and the questions were generally the same for parents and children. If the parents had partners (e.g., husband), they reported the average frequency of their and their partners’ media use.
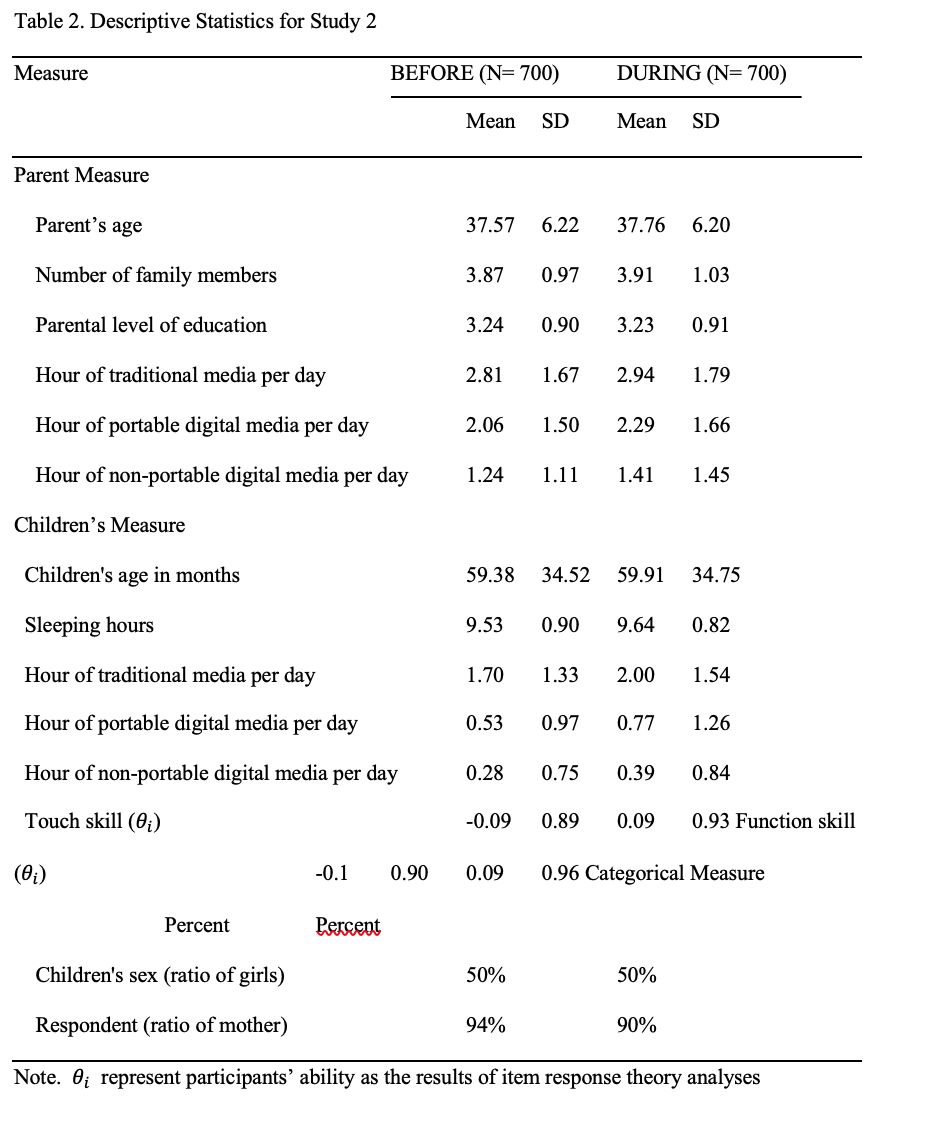
To assess the separate effect of each media on children’s skills, we classified media use into traditional media (TV and video), portable digital media (tablet computer and smartphone) and non-portable digital media (non-portable computer and non-portable game). We calculated the average hours per day of children’s use of each type of media for the analyses.
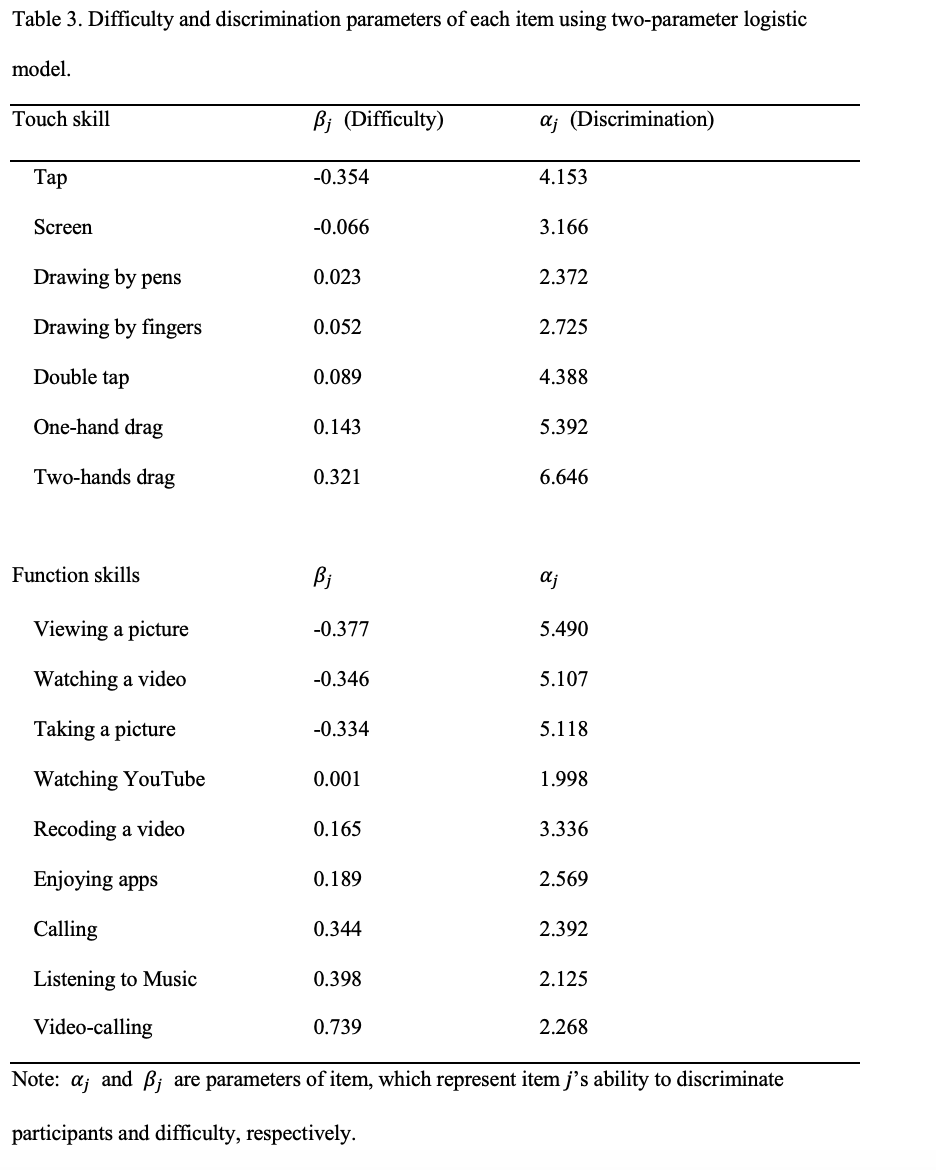
Skills to operate digital devices. Parents responded to questions about children’s skills for operating digital devices. We focused on touch skills and function skills that may show age-related changes between ages 0 to 9 (16, 28). We selected seven touch skills: tap, double tap, one-hand drag, two-hand drag, enlarge/reduce screen, drawing by fingers, and drawing by pens. Parents were asked to evaluate each of the children’s skills using a four-point scale (1. not at all, 2. very little, 3. somewhat, 4. to a great extent). In terms of function skills, we selected nine functions that can be used during early childhood based on the previous studies (29). The nine functions included viewing a picture, watching their own video, taking a picture, recording a video, watching YouTube, enjoying apps, call, video calling, and listening to music. Parents were asked to evaluate each of the children’s skills using a four-point scale (1. not at all, 2. very little, 3. somewhat, 4. to a great extent).
Analytic plan
Analyses were conducted in R (version 3.6, 1) using the irtoys (30) and lavaan packages. We conducted three analyses. First, we conducted item response theory analyses based on a two-parameter logistic model. That is, we converted the four-point scale data to a two-point scale data (we regarded 1 and 2 as zero, and 3 and 4 as one) and estimated item and ability parameters to separate the difficulty of each item in touch skills and function skills from each participants’ ability for touch skills and function skills. Using a two-parameter logistic model, a correct response rate of participant i, whose ability is θi, to item j Pj(θi) are modeled by the following equation.

Here, αj and βj are parameters of item 𝑗 which represents item 𝑗’s ability to discriminateθis and difficulty.
Second, in our preregistration, we planned to conduct a MANOVA. The analysis includes period (Before-pandemic and After-pandemic) and age (0 to 9) as independent variables and the duration of digital devices use for children and parents, and the touch skills and function skills as dependent variables. However, as in Study 1, many dependent variables were not normally distributed, and we could not conduct the planned MANOVA. Instead, we conducted SEM analyses considering non-normal distribution using maximum likelihood estimation to assess whether period and age affected the duration of digital devices use for children and parents, and the touch skills and function skills.
Finally, we conducted SEM analysis to assess the relationship between period and skills for digital devices, which was mediated by the duration of digital media use. Specifically, we used variables assessing the duration of digital media for the mediation analyses if we found significant main effects of period in the second analyses. We used demographic characteristics as control variables for the analysis.