Patient characteristics
A total of 62,294 patients with operable stage I-III colon cancer were finally included from the SEER data base as a training cohort (Supplementary Figure 1). In addition, 3,327 patients with operable stage I-III colon cancer from China Medical University Cancer Hospital were included as an external validation cohort. The characteristics of the baseline of the training and validation cohorts were presented (Supplementary Table 1). The mean ages (± SD) were 68.1 (± 13.8) and 59.9 (± 11.6) years in the training and validation cohorts, respectively. The mean number (± SD) of retrieved lymph nodes was 17.2 (± 9.6) and 16.7 (±10.0) in the training and validation cohorts, respectively. A total of 26.8% patients in the training cohort and 31.6% patients in the validation cohort had less than 12 retrieved lymph nodes.
LNR stages
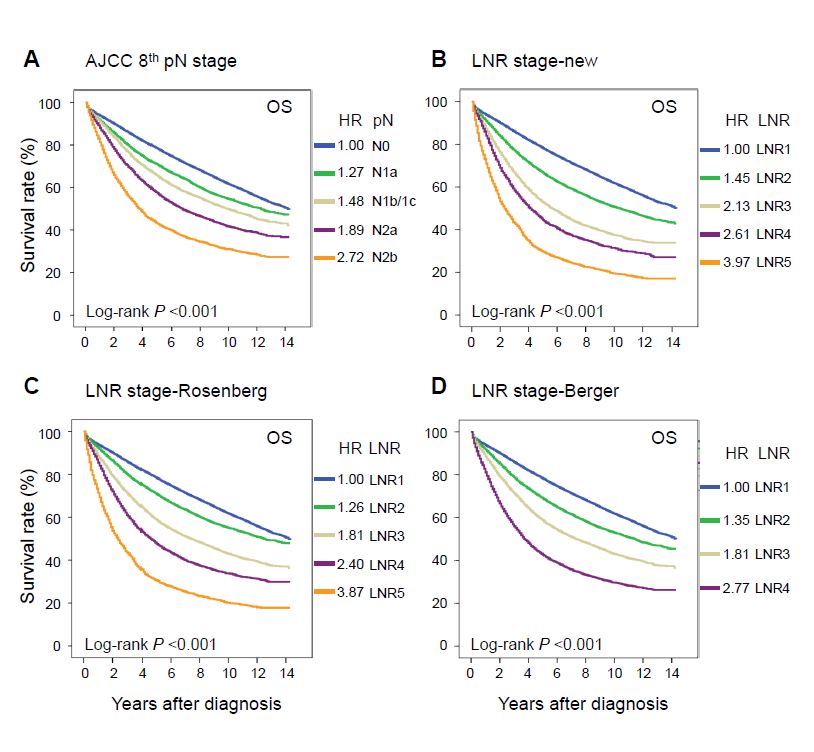
A novel LNR stage was established using four identified cutoff values (LNR, 0.05, 0.3, 0.5, and 0.7). Using these four cutoff values, we classified patients in the training cohort as follows: 0 ≤ LNR1 ≤ 0.05, 0.05 < LNR2 ≤ 0.3, 0.3 < LNR3 ≤ 0.5, 0.5 < LNR4 ≤ 0.7, and 0.7 < LNR5 ≤ 1 (Supplementary Table 2). There were two previous LNR stages which we named as LNR-Berger (Berger et al. 2005) and LNR-Rosenberg (Rosenberg et al. 2010). The cutoff values of these two LNR stages were: LNR-Berger (LNR, 0.05, 0.19, and 0.39) and LNR-Rosenberg (LNR, 0, 0.17, 0.41, and 0.69). Kaplan-Meier curves were presented to estimate the survivals of the AJCC 8th pN stage and these three LNR stages (Supplementary Figure 2).
TLNR classification
A novel TLNR classification was generated by combining the novel LNR and pT stages into 25 groups. Using these six identified cutoff values, we clustered patients of the 25 groups into seven clusters as follows: stage I (T1LNR1-2, T1LNR4), stage IIA (T1LNR3, T2LNR1-2, T3LNR1), stage IIB (T1LNR5, T2LNR3-4, T3LNR2, T4aLNR1), stage IIC (T2LNR5, T3LNR3-4, T4aLNR2, T4bLNR1), stage IIIA (T3LNR5, T4aLNR3-4, T4bLNR2), stage IIIB (T4aLNR5, T4bLNR3-4) and stage IIIC (T4bLNR5) (Table 1, Figure 1).
LNR stages versus the AJCC 8th pN stage
We compared the model discrimination performance and model-fitting ability of different LNR stages with the AJCC 8th pN stage in the training cohort. Compared to the AJCC 8th pN stage, all these three LNR stages showed significantly better prognostic discrimination (Hanley and McNeil test, all P < 0.001) and superior model-fitting ability (Supplementary Table 3). Similar findings were observed in patients with < 12 and ≥ 12 retrieved lymph nodes (Supplementary Table 3).
TLNR classification versus the AJCC 8th TNM classification
In the training cohort, model discrimination and model-fitting between the novel TLNR and the AJCC 8th TNM classifications were compared. Kaplan-Meier curves with log-rank tests confirmed that the novel TLNR classification showed superior model discrimination performance than the AJCC 8th TNM classification, that the 5-year overall survival rates of the TLNR classification steadily decreased as stage increased, and HRs increased as stage increased (HRs, TLNR stages I to IIIC, 1.00, 1.48, 2.13, 3.07, 4.87, 6.94, and 9.70) (Table 2, Figure 2A, 2B). The novel TLNR showed better prognostic discrimination (AUC, 0.621 vs. 0.608; Hanley and McNeil test, P < 0.001) and superior model-fitting ability (AIC, 561,129 vs. 562,052) than the AJCC 8th TNM classification for overall survival (Table 3). Similar findings were observed in patients with adequate (≥ 12) or inadequate (< 12) retrieved lymph nodes (Table 3). We further performed decision curve analyses to assess clinical utility, and the novel TLNR classification had superior net benefits over the AJCC 8th TNM classification between the threshold probabilities of 30–45% in the training cohort (Supplementary Figure 3A). The details of the novel TLNR and the AJCC 8th TMM classifications are presented (Figure 3).
External validation
In the external validation cohort, the TLNR still showed better model discrimination performance than the AJCC 8th TNM classification, that the 5-year overall survival rates of the TLNR classification steadily decreased as stage increased, and HRs increased as stage increased in both overall survival (HRs, TLNR stages I to IIIC, 1.00, 1.76, 2.54, 3.40, 6.35, 10.4, and 16.0) and disease-free survival (HRs, TLNR stages I to IIIC, 1.00, 2.46, 3.71, 4.94, 8.84, 13.8, and 18.1) (Table 2, Figure 2C, 2D, 2E, and 2F). The novel TLNR classification showed superior prognostic discrimination (AUC of overall survival, 0.646 vs. 0.604; AUC of disease-free survival 0.646 vs. 0.622, Hanley and McNeil test, all P < 0.001) than the AJCC 8th TNM classification (Table 3). Similar findings were observed in patients with inadequate lymph nodes retrieved (< 12) but not in patients with adequate lymph nodes retrieved (≥ 12), suggested the advantages of the novel TLNR classification, especially in patients with inadequate lymph nodes retrieved (Table 3). The decision curve analyses further revealed that the TLNR had superior net benefits over the AJCC 8th TNM classification between threshold probabilities of around 20–30% in overall survival and around 22–35% in disease-free survival (Supplementary Figure 3B, Supplementary Figure 3C).
A web tool was developed basing on the novel TLNR classification which could individually predict the overall survival (Figure 4, http://123.206.185.159:6070/).
{kind=link}
{kind=link}
{kind=link}