Inclusion and exclusion criteria for patients with suspected FH
Study design: observational, prospective, 2 years study (October 2017 to October 2019) at three academic medical centers in the North-Eastern part of Romania.
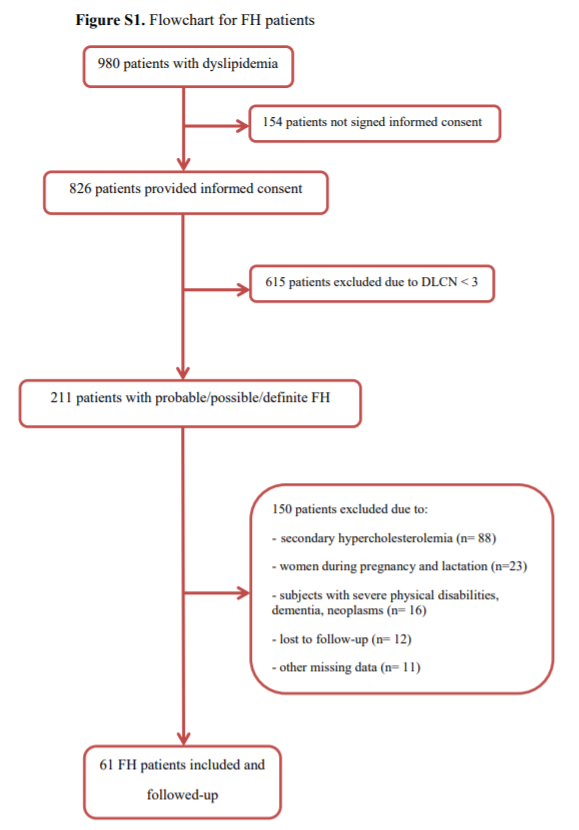
Study population: 980 patients with dyslipidemia were identified between September 2016 and October 2017, and 61 patients met the following inclusion criteria: subjects with full mental capacity who signed the informed consent form; men and women aged over 18 years. The DLCN score above 3 and the Simon Broome criteria (probable or possible FH) were two important selection tools for the patients with clinical diagnosis of FH. These included the following elements: identification of a family history of hypercholesterolemia or cholesterol deposits in vascular and extravascular tissues; setup of a personal history of early onset of coronary, cerebrovascular and peripheral vascular diseases; clinical observations regarding the presence of either xanthomas, xanthelasma and/or arcus cornealis; biological identification of total cholesterol (TC) > 300 mg/dL, low density lipoprotein cholesterol (LDL-C) > 190 mg/dL without treatment or > 100 mg/dL following treatment with maximum doses of statins (40 mg rosuvastatin, 80 mg atorvastatin, in combination with ezetimibe, as required) (Figure S1 flowchart for these patients).
Exclusion criteria: subjects lacking discernment or those who refused to sign the informed consent, patients under the age of 18, pregnant and breast-feeding women; subjects with severe physical disabilities, dementia, neoplasms and other causes of secondary hypercholesterolemia (uncontrolled diabetes, nephrotic syndrome, hypothyroidism, drug-induced dyslipidemia) [16] (Figure S1 flowchart for these patients).
Clinical and biological evaluation in FH patients
The follow-up included 3 components: clinical examination data, laboratory investigations and ultrasound parameters.
The study included patients with Dutch Lipid Clinic Network score >3 for the FH population [9]. The reference values of the DLCN score were: 3-5 points highlighted possible FH, 6-7 points indicated probable FH, while over 8 points indicated definite FH [9]. The other score, namely the Simon Broome score advertised between possible, probable or definitive FH [9]. The patients included in the study were coded with the letter H and the corresponding ID number.
Laboratory analysis included values at baseline, and at 12 and 24 months (stratified by statin alone- atorvastatin 80 mg maximum, rosuvastatin 40 mg, simvastatin 80 mg; combinations between high dose statin and ezetimibe 10 mg and/or fenofibrate 160 mg). Additionally, medical history revealed that certain patients had received antihypertensive medication (those with BP >140/90 mmHg), or oral antidiabetic medication (those diagnosed with type 2 diabetes), which was allowed throughout the study, according to the specialist doctors’ prescription.
The total cholesterol (TC) mg/dL, low density cholesterol lipoprotein (LDL-C) mg/dL, high density cholesterol lipoprotein (HDL-C) mg/dL, triglycerides (TG) mg/dL, blood glucose (mg/dL), aspartate transaminase (AST) U/L and alanine aminotransferase (ALT) U/L, uric acid (UA) mg/dL, high-sensitivity C-reactive protein (hsCRP) mg/dL were measured by spectrophotometric assay (UV VIS Spectrophotometer-Architect C8000- Abbott Laboratory, USA).
Further explorations for cardiovascular evaluation included:
- an electrocardiogram (ECG) for ischemic changes assessment;
- an ABI measurement with a sphygmomanometer and a portable ultrasonography device, which determines sounds that detect systolic blood pressure in the lower limbs; the reference ABI values were between 0.9 and 1.3.
- echocardiography (Siemens Acuson CV70 Cardiac Vascular Ultrasound Machine) highlighting left ventricular (LV) wall motion abnormalities and ejection fraction values, which are important predictors of left ventricular systolic dysfunction;
- measurement of cIMT (at the levels of carotid bifurcation, internal, external, right and left carotid arteries) by using Siemens Acuson CV70 Cardiac Vascular Ultrasound Machine, B-mode and color Doppler ultrasound (5-10 MHz). The average of the cIMT (the average of the six quantified segments) was also recorded. The reference cIMT values were under 0.9 mm [13, 17].
Evaluation of cardiovascular risk factors and the new cardiovascular events
Treatment goals were defined by the 2019 Guidelines on Dyslipidaemias [9]. The cardiovascular risk factors were defined according to the European Society of Cardiology (ESC): age and gender (> 50 years for men and > 60 years for women), genetic factors, race and ethnicity, diabetes mellitus (FPG ≥126 mg/dL: fasting was defined as no caloric intake for at least 8 h; 2-h plasma glucose≥200 mg/dL during oral glucose tolerance test: the test should be performed using a glucose load containing the equivalent of 75-g anhydrous glucose dissolved in water; A1C ≥6.5% using a standardized assay, classic symptoms of hyperglycemia or hyperglycemic crisis with a random plasma glucose ≥200 mg/dL), obesity (BMI exceeding 30 kg/m², waist circumference in Caucasian females >88 cm and in males > 102 cm), physical inactivity (under 30-60 min activity on most days), smoking (active or passive or without exposure to tobacco in any form) and high blood pressure (BP>140/90 mmHg) [9, 15, 18, 19].
Atherosclerotic cardiovascular disease (ASCVD) was defined as a history of one of the following diseases as identified in the medical records: coronary heart disease (CHD) with the following particularities: acute coronary syndrome, myocardial infarction (MI), stable angina, coronary revascularization, ischemic stroke, or transient ischemic attack and peripheral artery disease (PAD) [20].
Statistical analysis
The data of the patients with clinical diagnosis of FH were introduced into a database and processed through the statistical functions of the SPSS version 20.0 system. One-sample Kolmogorov-Smirnov for normal distribution tests were performed, with the data being calculated as: mean and standard deviation (SD) for normal distribution variables, percent for categorical variables by using a frequency test, median and interquartile range (IQR) for continuous variables with asymmetrical distribution. Bivariate correlation analysis was achieved between the scale variables, using the Pearson correlation coefficient. To analyze the associations between ordinary and/or nominal variables with specific variables, specific association coefficients were used (Cramer's, Phi, contingency coefficient). Comparative analyses between the pathological, family history, clinical and paraclinical history according to gender were performed for the values that did not meet the criteria of normal homogeneity, whereas normal distribution was performed for nonparametric tests: Mann-Withney U sample, Wilcoxon Signed-rank, Kruskall-Wallis H test, Friedman test. They were also employed for the categorical variables Chi Square (χ²) and Fisher Exact Test. Survival free of ASCVD, defined as cardiovascular events (CHD, stroke, PAD) during follow-up, was estimated using the Kaplan-Meier method. The duration of follow-up was calculated from the date of inclusion in the study to the date of the cardiovascular events. Multiple logistic regression analysis was applied to identify the independent factors for cardiovascular events. The P value <0.05 was considered statistically significant.
{kind=link}