Tables
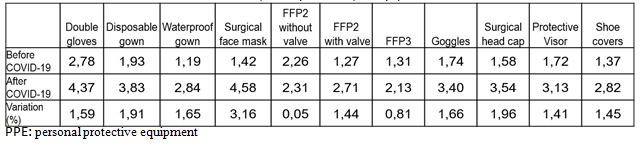
Tab. 1 Usual use of PPE before and after the onset of COVID-19
min 1(never)- max 5 (always)
Tab. 2. Usual use of PPE before and after the onset of COVID-19 for different healthcare workers
min 1 (never)- max 5 (always)
|
Nurse |
Doctor |
|||||||
|
PPE |
Before |
After |
Before |
After |
||||
|
Media |
St. Dev |
Media |
St. Dev. |
Media |
St. Dev. |
Media |
St. Dev. |
|
|
Double gloves |
3,88 |
1,09 |
4,40 |
1,15 |
2,50 |
1,07 |
4,39 |
0,96 |
|
Disposablegown |
2,16 |
1,03 |
3,80 |
1,32 |
1,87 |
1,04 |
3,86 |
1,20 |
|
Surgicalmask |
1,68 |
1,04 |
4,28 |
1,40 |
1,34 |
0,74 |
4,72 |
0,83 |
|
Waterproof gown |
1,25 |
0,64 |
3,17 |
1,47 |
1,16 |
0,41 |
2,78 |
1,33 |
|
FFP2 without valve |
2,39 |
1,08 |
2,72 |
1,28 |
2,23 |
1,03 |
2,23 |
1,21 |
|
FFP2 with valve |
1,30 |
0,63 |
3,04 |
1,55 |
1,25 |
0,56 |
2,64 |
1,35 |
|
FFP3 |
1,52 |
0,85 |
2,64 |
1,41 |
1,23 |
0,55 |
2,02 |
1,26 |
|
Surgical head cap |
2,12 |
1,01 |
3,92 |
1,35 |
1,64 |
0,99 |
3,43 |
1,31 |
|
Glasses |
1,88 |
0,93 |
3,52 |
1,29 |
1,48 |
0,88 |
3,39 |
1,28 |
|
Protectivevisor |
1,59 |
0,85 |
3,23 |
1,38 |
1,74 |
1,10 |
3,10 |
1,43 |
|
Shoe covers |
1,41 |
0,85 |
3,27 |
1,42 |
1,34 |
0,80 |
2,73 |
1,40 |
PPE: personal protective equipment
Tab. 3. Use of PPE in “suspected” and confirmed” case of COVID-19
|
CASE |
Double gloves |
Disposablegown |
Waterproof gown |
Surgicalfacialmask |
FFP2 without valve |
FFP2 with valve |
FFP3 |
Glasses |
Surgical head cap |
ProtectiveVisor |
Shoe covers |
|
Suspected |
96,24 |
83,33 |
85,04 |
71,82 |
56,64 |
73,83 |
41,24 |
92,13 |
94,49 |
82,79 |
76,27 |
|
Confirmed |
99,20 |
67,96 |
96,72 |
51,52 |
58,76 |
62,22 |
58,42 |
89,74 |
98,33 |
90,08 |
89,26 |
|
Variation (%) |
2,96 |
-15,37 |
11,68 |
-20,30 |
2,13 |
-11,61 |
17,18 |
-2,38 |
3,85 |
7,30 |
12,99 |
PPE: personal protective equipment
Tab. 4 Distribution of pediatric emergency room visits and hospitalizations rate
|
Pediatricemergency room visits march 2019 |
Pediatricemergency room visits march 2020 |
Reduction rate |
Pediatric recovery march 2019 |
Pediatric recovery march 2020 |
Reduction rate |
||
|
96.006 |
23.440 |
-72.566 |
75.58% |
11.968 |
3.780 |
-8.188 |
68.42% |