Results
We found 5826 articles after conducting our search in PubMed, EMBASE, Medline Ovid, Web of Science, Cochrane Central and Google Scholar. After removal of duplicates, 3771 articles remained. These articles were screened on title and abstract, after which 83 articles were included for full text screening. After full text screening, 65 articles were excluded. This resulted in 18 articles included for final data synthesis. (figure 1)
In the 18 articles that were included in this systematic review, a total of 35 combinations of biomarkers and clinical scoring systems were studied of which 33 unique combinations. In total, seven different clinical scoring systems and 21 different biomarkers were investigated. (table 1)
The Mortality in Emergency Department Sepsis (MEDS) score was the most used clinical scoring system, which was studied in 9 articles. The second most commonly used scoring system was the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, which was studied in 6 articles. The most commonly studied biomarker was PCT, which was studied in 7 articles. The combination of PCT with the MEDS score was the most studied combination of biomarker and clinical score and was studied in 3 different articles. There were no other combinations of biomarkers that were used by more than a single article.
The number of patients included in the studies ranged from 114 to 1318. The AUC of the combinations of biomarkers and clinical scoring systems ranged from 0,690 to 0,939. The highest AUC was achieved by the combination of Simplified Acute Physiology Score (SAPS II), PCT, lactate and interleukine-6 (IL-6), which yielded an AUC of 0,939 by Viallon et al.13, followed by the combination of SAPS-2 and soluble urokinase-type plasminogen activator receptor (suPAR) with an AUC 0.930 by Kofoed et al.14
Different inclusion criteria were used to classify patients as having sepsis. The most common criteria used were two SIRS criteria in combination with an infection, used by eight articles.13-20 The second most used inclusion criterion was the 2001 International Sepsis Definitions21, which was used by seven articles.17, 22-27 One article used the sampling of blood cultures as inclusion criterion.28 One article included patients with symptoms of systemic infection in which PCT or blood cultures were taken within 24 hours of admission.29 One article used the Sepsis-3 definition7 as inclusion criterion.30
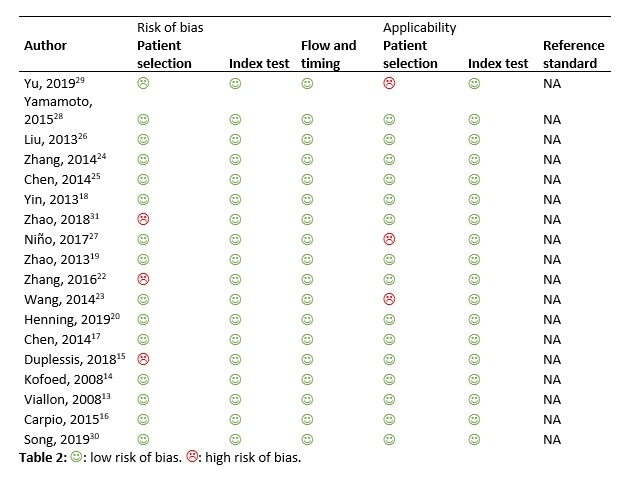
QUADAS-2 quality assessment
The quality assessment using the QUADAS-2 criteria can be found in table 2. Three studies were at risk of bias.15, 22, 31 These studies used multiple exclusion criteria, enrolling a very selected group of patients with sepsis. The exclusion criteria were mostly patients who were immunocompromised, for example due to immunosuppressant medication, malignancies or autoimmune diseases.22, 31
Only a minority of the articles used a predefined cutoff of the studied biomarkers and scoring system.17, 25, 27, 29
There were no concerns of possible bias in flow and timing of the biomarkers and scoring systems that were investigated. Blood sampling was performed during ED visit in all studies.
The studied population matched the review question in all but two studies. Nino et al.27 also included ICU patients and Koefoed et al.14 also included patients from a general ward along with ED patients. These studies were included nonetheless, because blood sampling occurred during admission.
Author, year |
Number of patients |
Biomarker 1 |
Biomarker 2 |
Biomarker 3 |
Clinical score 1 |
Clinical score 2 |
AUC |
|
Yu, 201929 |
1318 |
PCT |
qSOFA |
0,73 |
|||
|
CRP |
qSOFA |
0,69 |
|||||
|
Yamamoto, 201528 |
1262 |
CRP |
CURB65 |
0,77 |
|||
|
Liu, 201326 |
859 |
Presepsin |
|
MEDS |
0,731 |
||
|
Presepsin |
|
APACHE-2 |
0,734 |
||||
|
Zhang, 201424 |
680 |
Copeptin |
MEDS |
0,851 |
|||
|
Cortisol |
MEDS |
0,833 |
|||||
|
PCT |
Cortisol |
Copeptin |
MEDS |
0,891 |
|||
|
Chen, 201425 |
680 |
Lactate |
MEDS |
0,81 |
|||
|
Lactate |
APACHE-2 |
0,81 |
|||||
|
Lactate |
SOFA |
0,82 |
|||||
|
Yin, 201318 |
680 |
sTM |
MEDS |
0,805 |
|||
|
Zhao, 201831 |
655 |
PCT |
sPD-1 |
MEDS |
0,843 |
||
|
PCT |
MEDS |
0,792 |
|||||
|
sPD-1 |
MEDS |
0,829 |
|||||
|
Niño, 201727 |
563 |
TIMP1 |
MMP9 |
CHARLSON |
SOFA |
0,838 |
|
|
Zhao, 201319 |
501 |
PCT |
MEDS |
0,813 |
|||
|
Zhang, 201622 |
480 |
IgE |
APACHE-2 |
0,8 |
|||
|
IgE |
SOFA |
0,781 |
|||||
|
IgE |
MEDS |
0,89 |
|||||
|
Wang, 201423 |
480 |
NGAL |
MEDS |
0,858 |
|||
|
TIMP-1 |
MEDS |
0,882 |
|||||
|
PCT |
MEDS |
0,782 |
|||||
|
Henning, 201920 |
314 |
Angiopoientin-2 |
IL-6 |
0,72 |
|||
|
Chen, 201417 |
295 |
H-FABP |
MEDS |
0,853 |
|||
|
H-FABP |
APACHE-2 |
0,826 |
|||||
|
Troponine-I |
|
APACHE-2 |
0,811 |
||||
|
Troponine-I |
|
MEDS |
0,825 |
||||
|
Duplessis, 201815 |
203 |
Nucleosomes |
|
APACHE-2 |
0,84 |
||
|
Cell free DNA |
|
APACHE-2 |
0,81 |
||||
|
Kofoed, 200814 |
161 |
suPAR |
sTREM-1 |
SAPS-2 |
0,89 |
||
|
suPAR |
SAPS-2 |
0,93 |
|||||
|
Viallon, 200813 |
131 |
PCT |
IL-6 |
Lactate |
SAPS-2 |
0,939 |
|
|
Carpio, 201516 |
114 |
Presepsin |
|
MEDS |
0,878 |
||
|
Song, 201930 |
113 |
IL-6 |
PTX3 |
0,637 |
Table 1: Biomarkers. PCT: Procalcitonin, CRP: C-reactive protein, sTM: soluble thrombomodulin, sPD-1: soluble programmed death 1, TIMP-1: Tissue inhibitor of metalloproteinase-1, MMP9: Matrix metallopeptidase 9, NGAL: Neutrophil gelatinase-associated lipocalin, IL-6: interleukin-6, H-FABT: heart fatty acid binding protein, suPAR: soluble urokinase-type plasminogen activator receptor, PTX3: Pentraxin 3
Scoring systems. qSOFA: quick Sequential Organ Failure Assessment, MEDS: Mortality in Emergency Department Sepsis, APACHE-2: Acute Physiologic Assessment and Chronic Health Evaluation II, SOFA: Sequential Organ Failure Assessment, SAPS-2: Simplified Acute Physiology Score 2, CHARLSON