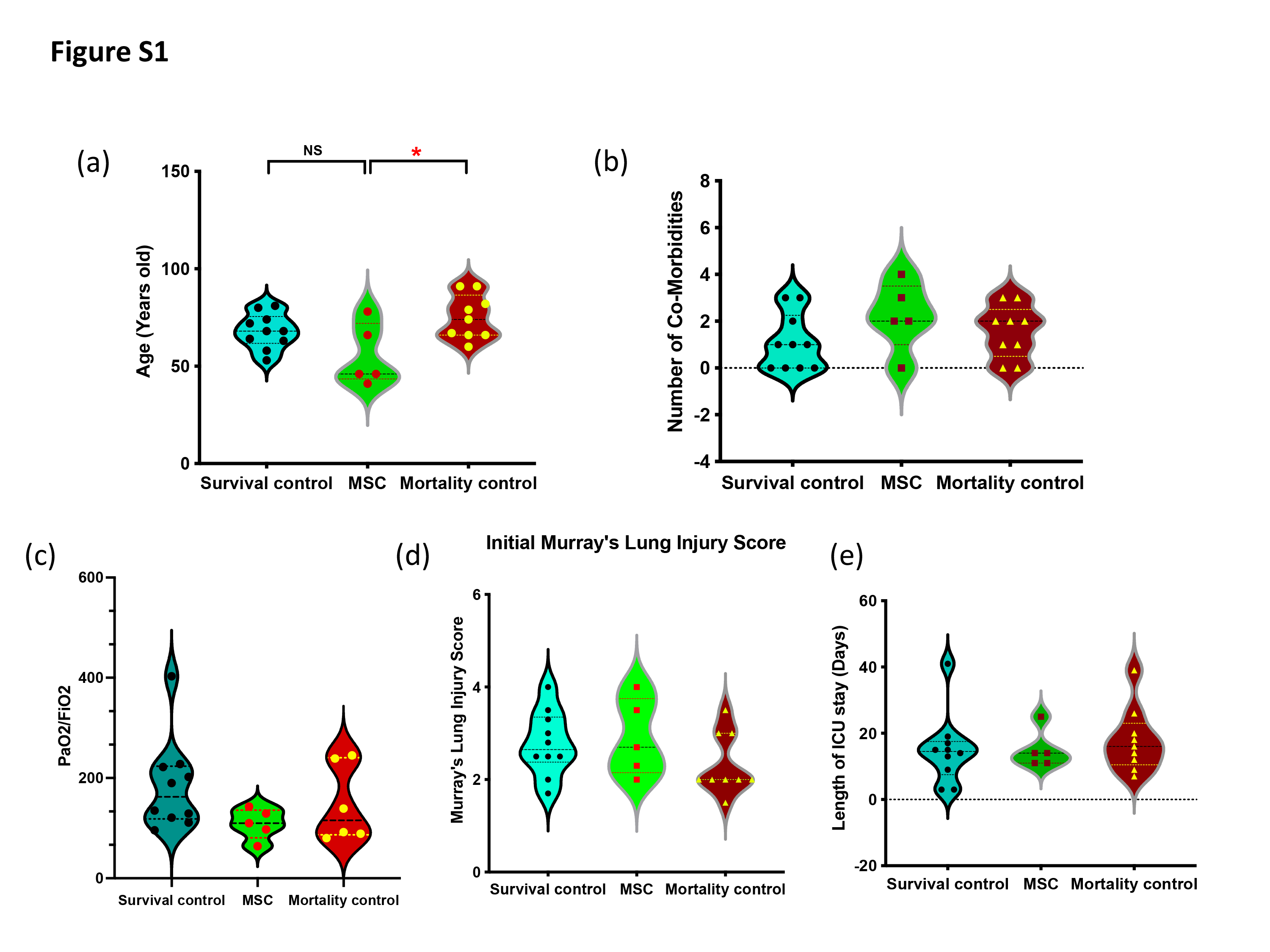
In this study, we have shown that pc-MSCs treatment was safe and effective in improving critically ill COVID19 patients with severe pneumonia. Nine out of 19 patients in the control group were documented in day-30 mortality marking 47% of deaths in our institution which was consistent with the reported mortality rate of ~50% of critically ill COVID patients [10]. There is no day-30 mortality in the pc-MSC treatment group and 2 out of 5 patients were able to prevent intubation, despite those patients having risk factors such as higher BMI and poor PaO2/FiO2 ratio.
Patients in both groups had high inflammation markers like C-reactive protein (CRP), D-dimer, Lactate dehydrogenase (LDH), ferritin as reported in COVID-19 cohorts [25, 26], even though patients had received anti-inflammatory agents, including dexamethasone and tocilizumab. Treatment with pc-MSC significantly inhibited hyper-inflammatory states by decreasing serum levels of ferritin, LDH and CRP.
It has been shown that SARS-CoV-2 RNAs, acting as pathogen-associated molecular patterns and sensing toll-like receptors, trigger downstream cascades in innate immune cells, resulting in the production of pro-inflammatory cytokines, such as (IL)-1β, IL-6 and interferon (IFN)-γ that induce synthesis of several defense proteins [27] from liver, including CRP, LDH and ferritin. These multi-functional peptides, especially LDH and ferritin levels are independent factors for predicting disease severity and mortality [28, 29]. Ferritin may activate nuclear factor-κB (NF-κB) [30], and create a vicious loop by further increase pro-inflammatory cytokines production, including IL-1β, IL-6 and IFN-γ, and contributing to the development of a cytokine storm syndrome. The decrease in serum levels of ferritin after pc-MSC treatment was associated with a concomitant decrease in IL-1β, IL-6 and IFN-γ serum levels, suggesting pc-MSC effectively broke the vicious cycle and attenuated cytokine storm syndrome. COVID-19 pneumonia severity was also significantly lessened in terms of Murray’s lung injury scores.
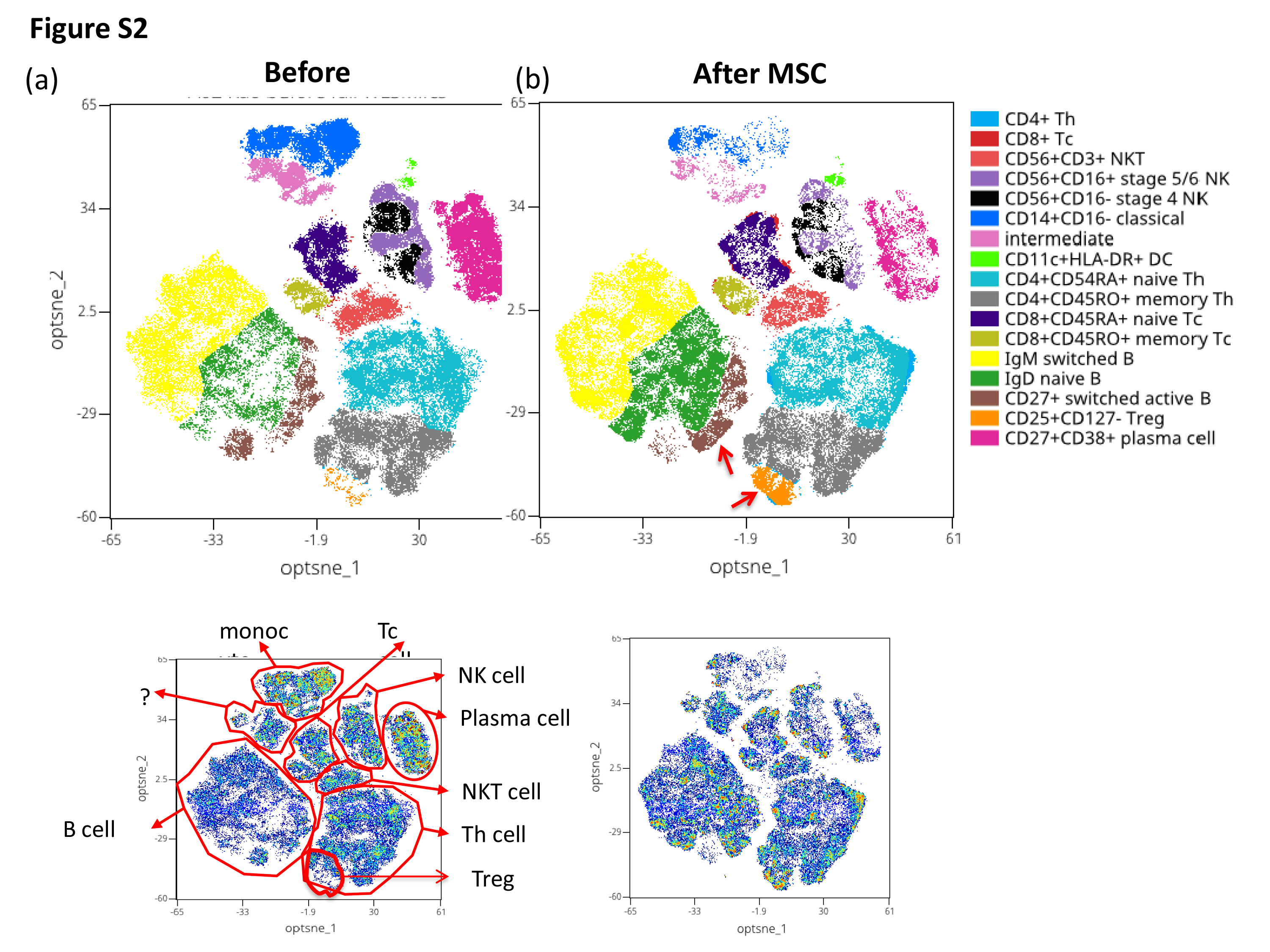
MSC therapy offers a promising treatment option for severe lung diseases caused by autoimmune, sepsis, and in COVID-19 infection [18-20]. The underlying cellular and molecular mechanisms of MSC-mediated immunomodulation, though still elusive, is proposed through a synergy of cell contact-dependent mechanisms and soluble factors [13, 31], via cytokine-dependent and cytokine-independent functional changes of monocytes/macrophages, dendritic cells, T cells, B cells, and natural killer cells [14, 15, 17, 32]. Peripheral blood immune profiles of the patients in the pc-MSC group were studied on days 0, 4 and 8 by using multi-parameter flow-cytometry analysis. TSNE cell clusters revealed a significant change in monocytes, Th cells, B cells, Treg cells and plasma/plasmablast cells subpopulations after pc-MSC treatment.
Monocytes and macrophages are the most important innate immune cells against viral infections. They mainly respond to SARS-CoV-2 infections by producing pro-inflammatory mediators through ACE2-independent and ACE2-dependent pathways to remove pathogens and repair tissue injury . However, dysregulation of their function such as through inappropriate activities to induce cytokine storm can result in the acute respiratory distress syndrome and other vital organs damage of the body including the heart [33]. During SARS-CoV-2 infection, circulating monocytes subpopulation, CD14+CD16+ monocytes, exhibits notable potency in contributing cytokine storms through producing a high level of TNF-α, IL-10, and IL-6 that are related to the deterioration of patients and increasing their admission to the ICU [2, 34]. The decrease in the absolute number of CD14+CD16+ subpopulation may be contributory to the attenuation of hyper-inflammation responses in the pc-MSC treatment group.
In severe COVID-19, lymphocytes are significantly reduced, and lymphopenia (absolute counts<1000 cells/μL) is considered an indicator for disease severity [35], therapeutic response [36], and disease outcome [37]. High levels of pro-inflammatory cytokines in cytokine storm such as TNF-α and IL-6 could induce lymphocyte deficiency [37]. All the patients in the pc-MSC treatment group had absolute lymphocyte counts <1000/ μL before treatment. The lymphocyte numbers in the peripheral blood significantly increased after treatment, probably due to the inhibitory effect of pc-MSC on pro-inflammatory cytokines, such as IL-6.
Lymphocytes in the peripheral blood including T cells, B cells and natural killer cells (NK cells) are critical to generate early control, viral clearance and disease resolution after SARS-CoV-2 infection [38, 39]. Regulatory T cells (Treg) play an important role in the prevention of excessive immune responses to SARS-CoV-2 infection [40]. Analysis of T lymphocyte subpopulations, patients of the pc-MSC treatment group had lower CD4+ and CD8+ T cell counts, butnot in the proportion of CD4+, CD8+ or Treg cells, compared with age-matched healthy controls. Treatment with pc-MSC significantly increased the proportion and absolute cell number of CD4+ T cells and Treg cells. Among CD4+ T cell subpopulations, memory T cells are crucial in viral clearance during the re-infection. Although the memory T cells were not identified as SARS-CoV2-specific, an increased number of memory T cell may suggest an adaptive immunity was being developed. MSCs have been shown to facilitate the formation of Treg cells [17, 41], via induction of Treg from conventional T cells [42, 43]. The increase in Treg cells is considered responsible for pc-MSC-mediated suppression of hyper-inflammatory responses in our patients. Additionally, MSC treatment has been shown to cause a shift from proinflammatory Th1 to anti-inflammatory Th2 cells [44]. Increased serum levels of IL-5, IL-4 and IL-13 after pc-MSC treatment may support this notion.
Effective immune response to SARS-CoV infection depends on the activation of CD8+ cytotoxic T cells through the killing of virus-infected cells [45]. However, although there was a trend for CD8+ T cells to increase with pc-MSC treatment, statistical significance was not reached. Our data about the role of NK cells in the pathogenesis of COVID-19 were limited. In one study there were no differences in the levels of NK cells among responders and non-responders before and following the treatment [46]. In another study, this trend was increasing among survivors and decreasing among non-survivors [47]. In our study, there was no significant change in NK cells after pc-MSC treatment.
B cells mediated antibody responses via coordination of other adaptive immune responses, including CD4+ T cells, CD8+ T cells are essential for effective control of COVID-19 infection [48]. B cells participate in the antiviral immune response by first rapidly releasing germline or near-germline antibodies from plasmablasts, via an extrafollicular pathway. Increased portions of IgM+ memory B cells and CD27+CD38+ plasma/plasmablast cells in the peripheral blood, compared to healthy controls, suggesting a protective memory response occurred in those patients with COVID-19 infection [5]. Upon appropriate cytokine stimulation, B cells undergo class switching and/or enter germinal centers within secondary lymphoid organs to undergo affinity maturation. This maturation process produces both long-lived plasma cells and memory B cells capable of responding to secondary challenge with homotypic or heterotypic antigenic challenge. Pc-MSC treatment significantly increased the proportion and absolute number of CD27+ switched activated B cells and concomitantly suppressed the proportion and absolute number of CD27+CD38+ plasma/plasmablast cells. These results suggest pc-MSC treatment shifted B cells from a protective memory response to COVID-19 infection to enhancing generation of virus-specific immunoglobulin switched B cells or long-lived plasma cells [49].
Limitation of this study:
The study was a small sample-sized study without true, randomized control group to provide strong evidence of treatment benefit. According to local government law and legislation, compassionate study for stem cell is limited to 3 patients. Due to pandemic issue, our study was performed up to 5 patients. At the time of treatment, all the patients were already treated with anti-viral and anti-inflammatory agents like Dexamethasone and Tocilizumab. The anti-inflammatory effect of pure Matriplax was hard to identify. Nevertheless, low mortality rate was noted at treatment group. In the control group, low anti-viral usage was due to local central disease control policy and drug regulation. Even so our interested patients were in severe condition and anti-viral has limited benefit on severe patients. Despite these limitations, we showed the desirable good prognosis in treatment group and biochemical response. Matriplax also balance dysregulation of immune response and it accelerated its homeostasis.
{kind=link}
{kind=link}
{kind=link}