Neoadjuvant chemotherapy (NAC), the standard of care for many breast cancer patients, is known to have systemic immunologic effects and is increasingly being used in clinical trials in combination with immunotherapeutics. Currently, there are few biomarkers to predict NAC or immunotherapy response, although response to NAC is known to be associated with long term outcome in breast cancer1. Thus, biomarkers are needed to identify patients who will benefit from combination therapy compared to those who are likely to respond to NAC alone, and thereby avoid the added risk of toxicity and financial burden. Peripheral blood is an attractive site of biomarker development due to the relative ease of longitudinal sampling. We have previously shown that high expression of a cytotoxicity gene signature in the blood following NAC is associated with the presence of residual disease (RD) and future breast cancer recurrence, demonstrating the feasibility of using blood-based transcriptional biomarkers2.
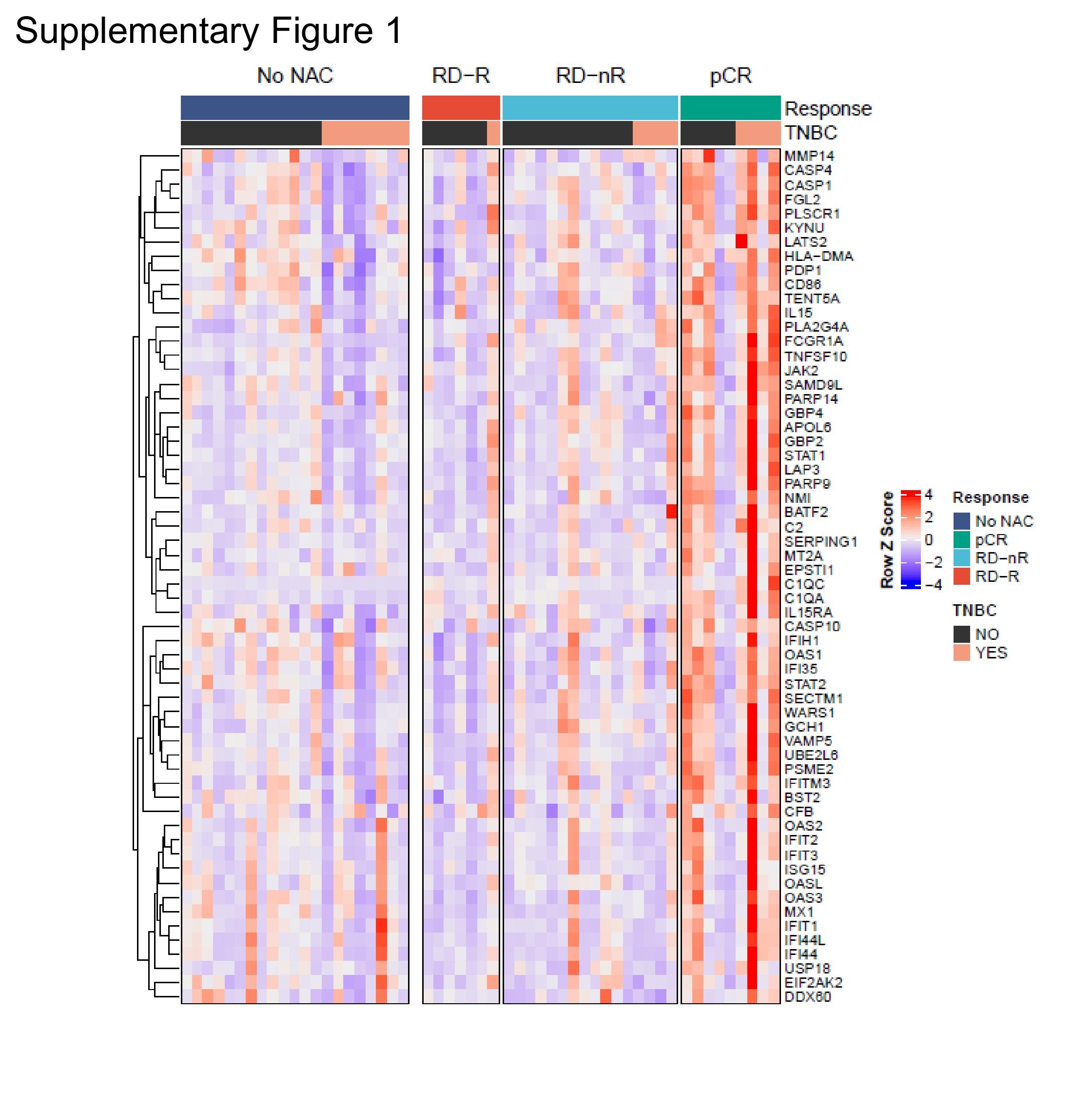
RNA sequencing was performed on whole blood of 53 breast cancer patients after completion of NAC (if received) and prior to definitive surgery (Fig. 1a; n=23 RD, 9 pathologic complete response (pCR), 21 no NAC; Table 1). We stratified patients with RD by whether they experienced a breast cancer recurrence within three years of surgery (RD-R) or remained free of recurrence for three years (RD-nR). Using DeSeq, we identified 1,238 (FDR corrected q-value <0.1) differentially expressed genes between pCR and RD samples (Supplemental Table 1)3. Using gene set enrichment analysis (GSEA), we collapsed differentially expressed genes into pathways using the Molecular Signatures Database hallmark gene sets4,5. Hallmark Interferon (IFN) Gamma Response (q-value <0.0001; normalized enrichment score (NES)=3.32), Hallmark Interferon Alpha Response (q-value <0.0001; NES=3.14), and Hallmark Complement (q-value=0.000111; NES=2.29) pathways were significantly enriched in the blood of patients experiencing pCR compared to those with RD (Fig. 1b). No pathways were statistically significantly upregulated in RD samples relative to pCR samples. To evaluate the genes involved in these pathways, we identified the leading-edge genes from each pathway (IFN gamma = 49 genes; IFN alpha = 26 genes; complement = 15 genes) and selected only the unique genes (n=60 genes). There is strong, uniform upregulation of many of these genes in many of the pCR samples, regardless of TNBC status (Supplementary Fig. 1). We combined expression of these genes into an IFN/complement score, calculated as sum of z-scores divided by number of genes in the signature (n=60 genes). We compared expression of the IFN/complement score to a previously published 8 gene cytotoxic score (FGFBP2 + GNLY + GZMB + GZMH + NKG7 + LAG3 + PDCD1 – HLA-G)2. No genes overlapped between the two signatures. Samples with the highest expression of the IFN/complement had low expression of the cytotoxic score and tended to be pCR samples. Conversely, those with highest expression of the cytotoxic score tended to have low expression of the IFN/complement score and be RD samples (Fig. 1c). A combination peripheral immunologic response score (PIRS) of IFN/complement score minus cytotoxic score had improved predictive power compared to either signature alone (Fig. 1d). To examine which cell types predominately express each signature, we used single cell RNA sequencing data from whole peripheral blood mononuclear cells (PBMCs) from two breast cancer patients post-NAC, prior to surgery2. Expression of the cytotoxic score was the highest in CD8+ T cells and natural killer cells, while the IFN/complement score was the highest in a subset of monocytes. There was very little co-expression of the signatures across cells (Fig. 1e).
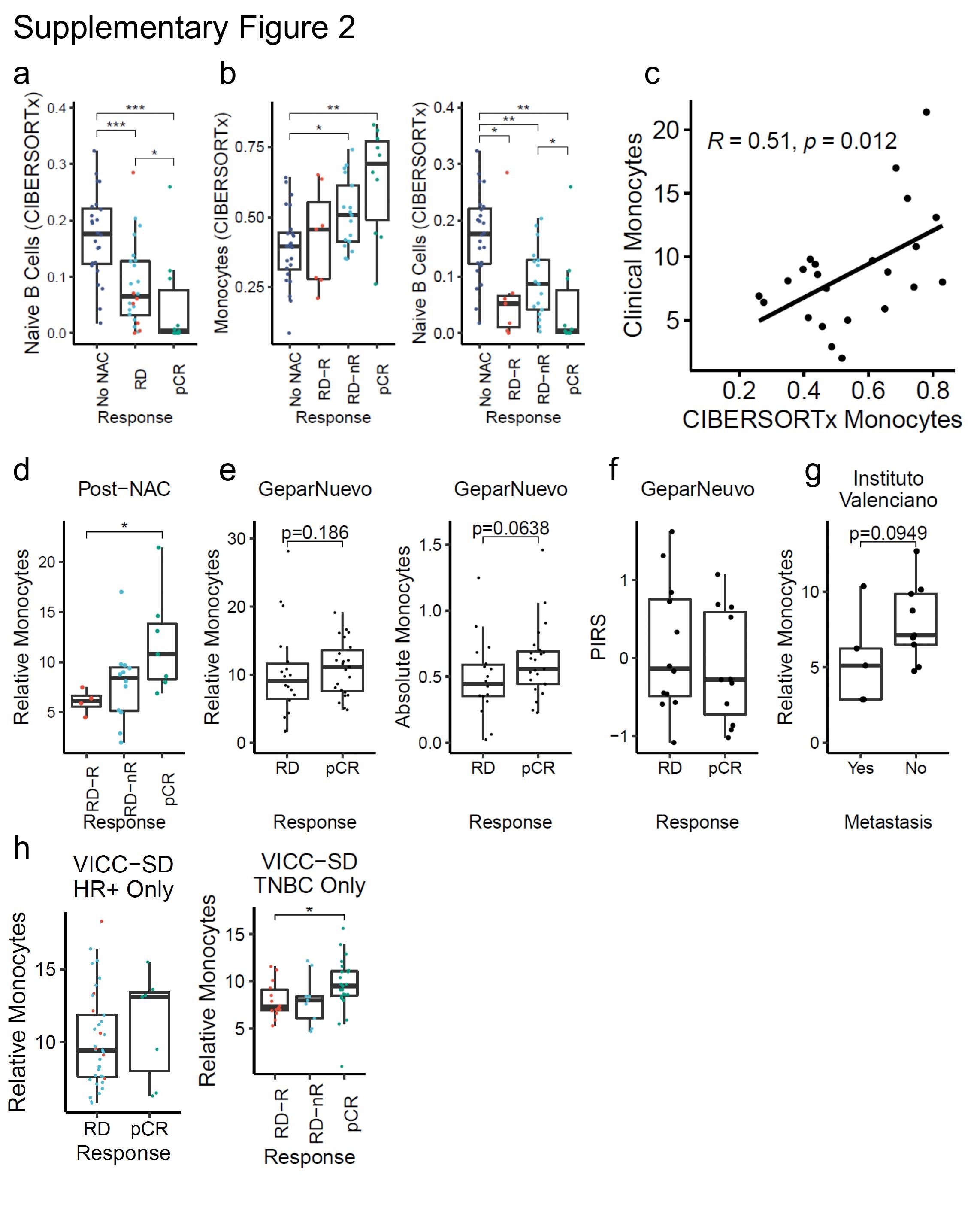
Given the partitioning of the gene expression scores into cell types, we next aimed to identify whether there were differences in cell type abundances between the outcome groups. CIBERSORTx was used to deconvolute relative cell type abundance from the RNA sequencing data6 (Fig. 2a). Relative monocyte abundance was highest in samples with pCR, intermediate in those with RD, and lowest in samples not receiving NAC (Fig. 2b). Naïve B cells were also statistically significantly different across groups, being highest in no NAC samples and lowest in pCR samples (Supplementary Fig. 2a). However, only monocytes followed the trend of increases from no NAC to RD-R to RD-nR to pCR (Supplementary Fig. 2b). Additionally, the routine nature of clinically measuring monocytes made monocyte values an intriguing metric for further study. We reviewed electronic medical records and extracted monocyte values from complete blood counts for patients receiving NAC in this cohort. 23 out of 32 (72%) of NAC-treated patients (n=7 pCR, 12 RD-nR, 4 RD-R) had a complete blood count with differential (which includes monocyte values) in the 30-day interval prior to surgery (following completion of NAC), indicating the commonality of collecting this information clinically. Clinically measured monocyte values were significantly positively correlated with monocyte values inferred by CIBERSORTx (R=0.51, p=0.012; Supplementary Fig. 2c), even though monocyte values were not always collected on the same day as the blood for RNA sequencing (though in the same 30-day window). Post-NAC, but not pre-NAC, monocytes were significantly higher in patients with pCR compared to those with RD (Fig. 2c; Supplementary Fig. 2d).
Next, we sought to assess whether monocyte abundance was associated with outcome in independent cohorts. Higher monocytes were also seen with pCR in an additional cohort of 41 TNBC patients (n=18 RD, 23 pCR; placebo arm of the GeparNuevo study; Table1), though this association was not statistically significant (p=0.0638 for absolute monocyte counts, p=0.186 for relative monocyte frequencies, one-tailed Wilcoxon; Supplementary Fig. 2e)7. In this TNBC only dataset PIRS, measured by NanoString, was not associated with outcome, indicating independence of monocytes and PIRS measurements (Supplementary Fig. 2f). In an additional independent cohort of 14 hormone receptor positive (HR+) HER2- breast cancer patients from the Instituto Valenciano de Oncología, monocytes tended to be higher in patients without metastatic recurrence, with at least four years of follow-up time for each patient (p=0.0949, one-tailed Wilcoxon; n= 5 with metastasis, 9 without metastasis; Supplementary Fig. 2g; Table 1). Using a de-identified medical record database called the synthetic derivative (SD), we identified 110 breast cancer patients (VICC-SD; n=35 pCR, 75 RD; Table 1) who had been treated with NAC, had a breast surgery, and had a monocyte value within 30 days prior to surgery. In the VICC-SD cohort, relative frequencies of monocytes were statistically significantly higher in patients with pCR compared to those with RD (Fig. 2d). This effect was more pronounced when considering only the TNBC patients (n=50), which may be reflective of underlying TNBC-specific biology, or the more uniform treatment options for TNBC (chemotherapy rather than targeted therapy agents) (Supplementary Fig. 2h). In all cohorts, patients who had received GM-CSF products in the 30-day window prior to surgery were excluded from analysis as this may affect monocyte counts. Taken together, these data suggest that higher blood monocyte levels post-NAC may be indicative of superior outcomes in breast cancer patients.
Peripheral blood gene expression scores and cell type abundance may be useful biomarkers of NAC response and outcomes in breast cancer. We identified an immunologic gene signature (PIRS) that was highest in patients with the best outcomes (pCR) and lowest in those with the worst outcome (RD with recurrence). However, PIRS was not associated with outcome in a separate cohort of TNBC only patients. Additional studies are needed to test whether PIRS or other gene expression scores may be useful biomarkers in breast cancer patients. Higher peripheral monocytes, a standard clinical assay performed on most breast cancer patients, was associated with improved patient outcomes (pCR or lack of recurrence) in four independent breast cancer patient cohorts. Additional efforts are needed to explore whether there might be a causal link between chemotherapy induced monocyte mobilization and improved response. Taken together, these results suggest that peripheral blood biomarkers following NAC may be useful in predicting long-term outcome. Future work will explore the utility of peripheral blood biomarkers in predicting immunotherapy response.
{kind=link}
{kind=link}