Comparison of lymphocyte subsets between AGCs and NCs
The following comparison was performed to analyze the injury status of PL and ACL in AGCs. The PL and ACL in AGCs and NCs were detected and compared. Compared with NCs, the PL of AGCs were decreased only in CD3+CD8+ and B cells (P = 0.022; P = 0.004, respectively) (Fig. 2A), while the ACL in AGCs were all significantly decreased (P < 0.001) (Fig. 2B).
Compared to NCs, we found a more regular pattern of impairment in ACL than PL in AGCs.
Comparison Of Pl And Acl In Agcs Between Stage Ⅲ And Stage Ⅳ
We further analyzed the changes in the PL and ACL at different stages of AGCs.
More importantly, when analyzing the relationship between PL, ACL, and clinical stage, only the percentage of CD3+CD8+ and B cells were different in AGCs with stage III compared with NCs (P = 0.032; P = 0.036, respectively) (Fig. 2C), while the ACL in AGCs with stage III were all significantly different from that of NCs (P < 0.001) (Fig. 2D). When comparing AGCs with stage Ⅳ to NCs, only the percentage of B cells in AGCs was different (P = 0.005) (Fig. 2E), and the ACL of AGCs was all significantly different from that of NCs too (P < 0.001) (Fig. 2F). The PL had no significant difference in AGCs between stage Ⅲ and stage Ⅳ (P > 0.05) (Fig. 2G), however, the ACL in AGCs with stage Ⅳ decreased significantly (CD3+, P < 0.001; CD4+, P < 0.001; CD8+, P < 0.001; B, P < 0.001; NK, P = 0.001, respectively) (Fig. 2H).
This result suggested that the decreases of ACL in AGCs were more significant and sensitive to reflect the injury of lymphocyte subsets than PL. Only attention was paid to PL in clinical practice, it could lead to clinical misjudgment and affect treatment. The PL represents the proportion and composition of lymphocyte subsets[24], which directly reflects their development and differentiation function, while ACL was an exact number, direct reflecting their proliferation ability[25]. These results suggested that the impaired proliferation of lymphocyte subsets in peripheral blood of AGCs may be an important reason for the progression of GC.
Prognostic Impact Of Acl On Pfs
We analyzed the relationship between ACL and PFS of AGCs. The PFS of AGCs with stage III was significantly higher than that of AGCs with stage IV (HR 0.26; 95%CI [0.18–0.38]; P < 0.0001) (Fig. 3A). To further analyze the effect of ACL on PFS, the cut-off points of ACL were analyzed and calculated by the ROC curve (Table 2). The results suggested that the AC of each subgroup of lymphocytes was higher than the cut-off point, and the PFS of AGCs was significantly longer. The AC was lower than the cut-off point, and the PFS was significantly shorter, which showed a significant positive correlation. The related results of CD3+, CD3+CD4+, CD3+CD8+, B and NK cells were shown in Fig. 3B (HR 5.04; 95% CI [3.47–7.31]; P < 0.0001), Fig. 3C (HR 9.25; 95% CI [6.44–13.26]; P < 0.0001), Fig. 3D (HR 2.16; 95% CI [1.51–3.10]; P < 0.0001), Fig. 3E (HR 2.05; 95% CI [1.43–2.95]; P < 0.0001) and Fig. 3F (HR 2.39; 95% CI [1.67–3.43]; P < 0.0001), respectively.
Thus, the PFS of AGCs reduced as GC progressed and distant metastasis occurred. Peripheral blood ACL was closely related to the prognosis of PFS in AGCs. The higher the ACL, the better the prognosis, otherwise, the poorer the prognosis. This suggested that the number of lymphocyte subsets was the basis for normal immune function and it showed that high ACL was conducive to improving the PFS of AGCs.
Prognostic Impact Of Acl On Os
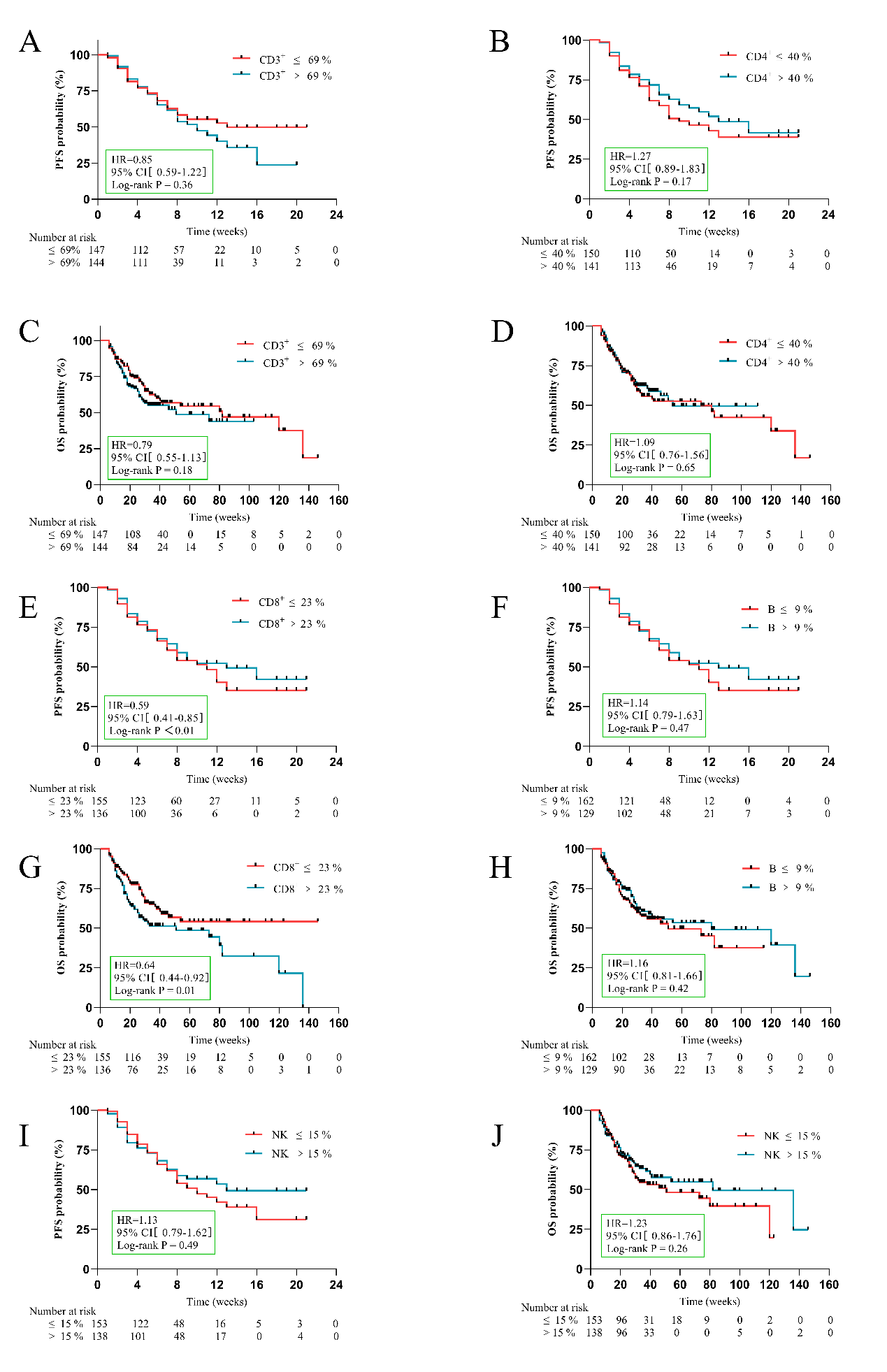
We also analyzed the relationship between ACL and OS of AGCs. Figure 4A showed that OS was significantly higher with stage III than that in AGCs with stage IV (HR 0.25; 95%CI [0.18 to 0.36]; P < 0.0001). Similar to PFS, AGCs with CD3+ > 652 cells/µL (Fig. 4B, HR5.13; 95%CI [3.53 to 7.45]; P < 0.0001), CD3+CD4+ > 405 cells/µL ( Fig. 4C, HR9.61; 95%CI [6.70 to 13.80]; P < 0.0001), CD3+CD8+ > 215 cells/µL (Fig. 4D, HR2.41; 95%CI [1.68 to 3.46]; P < 0.0001), B > 77 cells/µL (Fig. 4E, HR2.19; 95%CI [1.52 to 3.14]; P < 0.0001) and NK > 140 cells/µL (Fig. 4F, HR2.57; 95%CI [1.79 to 3.69]; P < 0.0001), their OS were significantly longer than those of AGCs with lower ACL than cut-off point of their itself, respectively. Prognostic impacts of PL on PFS and OS had no significant difference (P > 0.05) (Supplement Fig. 1), except for the percentage of CD3+CD8+ (Supplement Fig. 1E and 1G).
The OS of AGCs was closely related to the ACL, so high numbers of lymphocytes could prolong the OS of AGCs.
Effect Of Variables On The Pfs And The Os Of Agcs
As there were five subsets of ACL that affected PFS and OS of patients, it was necessary to analyze and evaluate which ACL was the best prognostic biomarker for AGCs. Univariate analysis and Log-rank test were used to analyze the variables (Table 2), and then the variables of P < 0.05 were input to multivariate analysis for COX model analysis (Fig. 5). In Fig. 5A, higher AC of CD3+CD4+ cells (> 405 cells/µL) (HR 0.192; 95%CI [0.092 to 0.398]; P < 0.001) was an independent protective factor for PFS, while clinical stage IV (HR 2.433; 95%CI [1.513to3.911]; P < 0.001) and family history (HR 1.603; 95%CI [1.053 to 2.441]; P = 0.028) was an independent risk factor for PFS. In Fig. 5B, higher AC of CD3+CD4+ cells (> 405 cells/µL) (HR 0.196; 95%CI [0.093 to 0.411]; P < 0.001) was an independent protective factor for OS, while clinical stage IV (HR 2.288; 95%CI [1.411 to 3.71]; P = 0.001) was an independent risk factor for OS.
This indicates that the AC of CD3+CD4+ cells is the best prognostic biomarker of PFS and OS of AGCs.
Table 2
Univariate analysis of PFS and OS of AGCs
| Univariate viable Cutoff point PFS OS |
| | | p-value | HR | p-value | HR |
| Age (≥ 66 vs < 66) (years) | 66 | 0.271 | 1.225 | 0.380 | 1.176 |
| Sex (Male vs Female) | | 0.308 | 0.806 | 0.177 | 0.751 |
| Family history (Yes vs No) | | 0.025 | 1.581 | 0.061 | 1.465 |
| Past medical history (Yes vs No) | | 0.960 | 1.009 | 0.429 | 1.158 |
| Smoking history (Yes vs No) | | 0.726 | 1.071 | 0.503 | 1.141 |
| Drinking history (Yes vs No) | | 0.936 | 0.985 | 0.779 | 0.949 |
| Adenocarcinoma (Yes vs No) | | 0.772 | 0.935 | 0.872 | 1.038 |
| Differentiated degree (Moderate or High vs Low) | | 0.100 | 0.615 | 0.105 | 0.618 |
| Clinical stage (Ⅳ vs Ⅲ) | | < 0.001 | 3.934 | < 0.001 | 4.360 |
| Lymph node metastasis (Yes vs No) | | 0.289 | 1.241 | 0.232 | 1.280 |
| CD3 + cell (%) (High vs Low) | 69 | 0.375 | 1.178 | 0.187 | 1.279 |
| CD4 + cell (%) (High vs Low) | 40 | 0.189 | 0.784 | 0.657 | 0.920 |
| CD8 + cell (%) (High vs Low) | 23 | 0.004 | 1.712 | 0.014 | 1.578 |
| B cell (%) (High vs Low) | 9 | 0.490 | 0.879 | 0.421 | 0.860 |
| NK cell (%) (High vs Low) | 15 | 0.509 | 0.885 | 0.267 | 0.813 |
| AC of CD3 + cell (cells/µL) (High vs Low) | 625 | < 0.001 | 0.192 | < 0.001 | 0.190 |
| AC of CD4 + cell (cells/µL) (High vs Low) | 405 | < 0.001 | 0.100 | < 0.001 | 0.098 |
| AC of CD8 + cell (cells/µL) (High vs Low) | 215 | < 0.001 | 0.462 | < 0.001 | 0.411 |
| AC of B cell (cells/µL) (High vs Low) | 77 | < 0.001 | 0.484 | < 0.001 | 0.447 |
| AC of NK cell (cells/µL) (High vs Low) | 140 | < 0.001 | 0.415 | < 0.001 | 0.385 |
Prognosis Of Acl On Pfs And Os In Agcs Received Chemotherapy
To evaluate the prognosis of lymphocyte subsets on PFS and OS in AGCs received chemotherapy, we analyzed the prognosis between lymphocyte subsets and PFS and OS of 93 AGCs who received chemotherapy (Table 3).
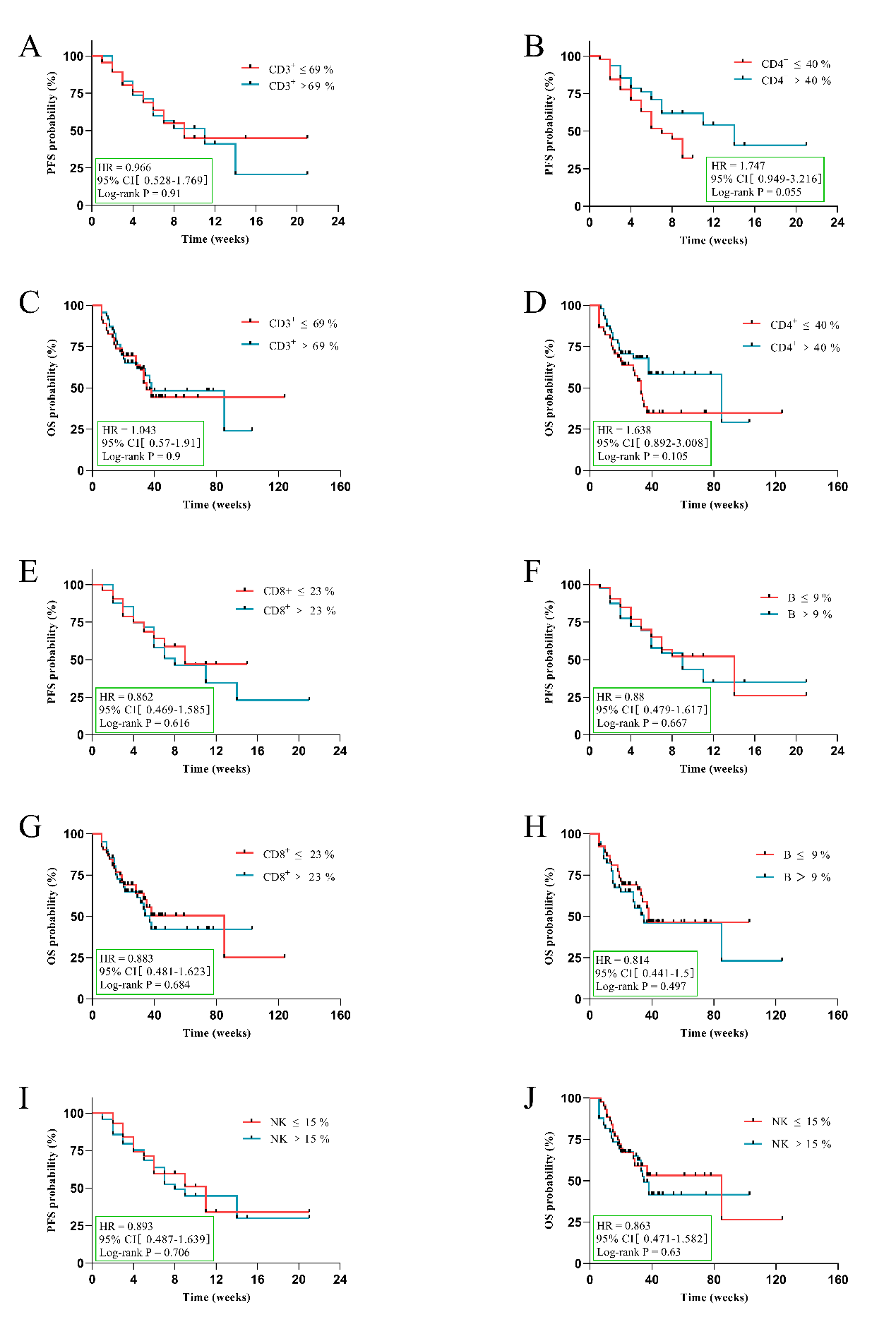
Similar to the previous results, AGCs received chemotherapy with higher AC of CD3+, CD3+CD4+, CD3+CD8+, B, and NK cells had significantly longer PFS and OS than those of AGCs with lower ACL than the cut-off point of their itself. The related PFS and OS results of CD3+, CD3+CD4+, CD3+CD8+, B and NK cells were shown in Fig. 6A, HR 4.268, 95%CI [0.231 to 8.166], P < 0.0001; Fig. 6B, HR 5.337, 95%CI [2.884 to 9.877], P < 0.0001; Fig. 6C, HR 2.612, 95%CI [1.419 to 4.808], P = 0.0016; Fig. 6D, HR 1.896, 95%CI [1.026 to 3.505], P = 0.03; Fig. 6F, HR 4.657, 95%CI [2.408 to 9.007], P < 0.0001; Fig. 6G, HR 5.337, 95%CI [2.884 to 9.877], P < 0.0001; Fig. 6H, HR 3.228, 95%CI [1.733 to 6.015], P < 0.0001; Fig. 6I, HR 2.215, 95%CI [1.141 to 3.955], P = 0.01; Fig. 6J, HR 1.802, 95%CI [0.972 to 3.339], P = 0.0473, respectively; excepted AC of NK cells in PFS (Fig. 6E, HR 1.657, 95%CI [0.9 to 3.06], P = 0.09). And there was no significant difference in the prognostic effect of PL on PFS and OS in AGCs received chemotherapy (P > 0.05) (Supplement Fig. 2).
Given this, to determine which ACL has the most significant prognosis on the PFS and OS of AGCs received chemotherapy, we conducted univariate (Table 4) and multivariate analyses (Fig. 7). Higher CD3+CD4+ cells (> 405 cells/µL) (HR 0.272; 95%CI [0.086 to 0.861]; P = 0.027) was an independent protective factor for PFS and OS in AGCs.
Therefore, a higher ACL was a prerequisite and basis for chemotherapy to prolong the survival of AGCs, especially a higher AC of CD3+CD4+ cells.
Table 3
The baseline characteristics of AGCs received chemotherapy.
| Characteristics | N = 93 | % |
| Age (years) | | |
| ≤ 66 | 51 | 55 |
| > 66 | 42 | 45 |
| Sex | | |
| Male | 66 | 71 |
| Female | 27 | 29 |
| Family history | | |
| Yes | 22 | 23.7 |
| No | 71 | 76.3 |
| Smoking history | | |
| Yes | 46 | 49.5 |
| No | 47 | 50.5 |
| Drinking history | | |
| Yes | 20 | 21.5 |
| No | 73 | 78.5 |
| Adenocarcinoma | | |
| Yes | 55 | 59.1 |
| No | 38 | 40.9 |
| Differentiated degree | | |
| Low | 77 | 82.8 |
| Medium or High | 16 | 17.2 |
| Clinical stage | | |
| Ⅲ | 35 | 37.6 |
| Ⅳ | 58 | 62.4 |
| Lymph node metastasis | | |
| Yes | 25 | 26.9 |
| No | 68 | 73.1 |
| Response evaluation | | |
| Complete response (CR) | 0 | 0 |
| Partial response (PR) | 11 | 11.8 |
| Stable disease (SD) | 40 | 43 |
| Progressive disease (PD) | 42 | 45.2 |
Table 4
Univariate analysis of PFS and OS of AGCs received chemotherapy
| Univariate viable Cutoff point PFS OS |
| | | p-value | HR | p-value | HR |
| CD3 + cell (%) (High vs Low) | 69 | 0.911 | 1.035 | 0.891 | 0.959 |
| CD4 + cell (%) (High vs Low) | 40 | 0.068 | 0.555 | 0.113 | 0.609 |
| CD8 + cell (%) (High vs Low) | 23 | 0.628 | 1.162 | 0.688 | 1.133 |
| B cell (%) (High vs Low) | 9 | 0.678 | 1.137 | 0.503 | 1.231 |
| NK cell (%) (High vs Low) | 15 | 0.715 | 1.121 | 0.635 | 1.161 |
| AC of CD3 + cell (cells/µL) (High vs Low) | 625 | < 0.001 | 0.212 | < 0.001 | 0.195 |
| AC of CD4 + cell (cells/µL) (High vs Low) | 405 | < 0.001 | 0.178 | < 0.001 | 0.156 |
| AC of CD8 + cell (cells/µL) (High vs Low) | 215 | 0.003 | 0.380 | < 0.001 | 0.285 |
| AC of B cell (cells/µL) (High vs Low) | 77 | 0.04 | 0.526 | 0.015 | 0.460 |
| AC of NK cell (cells/µL) (High vs Low) | 140 | 0.102 | 0.601 | 0.053 | 0.541 |
Based on previous analysis, the ACL was divided into high and low groups according to their cutoff point (Table 5). In 93 patients, 47 (51%) had a high AC of CD3+CD4+ (> 405 cells/µL), of them 11 (24%) were PR, 26 (55%) were SD, 10 (21%) were PD, the DCR reached 79%, while 46 (49%) had a low AC of CD3+CD4+ (≤ 405 cells/µL), of them 0 were PR, 14 (30%) were SD, 32 (70%) were PD, the DCR was 30% only. The AC of CD3+, CD3+CD8+, B, and NK cells showed similar characteristics to the AC of CD3+CD4+. The higher ACL (> cutoff-point) had better DCR than the lower ACL (≤ cutoff-point), which means the lower ACL had a higher PD rate.
Table 5
Evaluation response of ACL of AGCs received chemotherapy
| Cells | Groups | n | Disease control | Progressive Disease |
| | | 93 | PR = 11 | SD = 40 | PD = 42 |
| n (%) | n (%) | n (%) |
| CD3+ | > 625 cells/µL | 56 | 11 (20%) | 32 (57%) | 13 (23%) |
| ≤ 625 cells/µL | 37 | 0 | 8 (22%) | 29 (78%) |
| CD3+CD4+ | > 405 cells/µL | 47 | 11 (24%) | 26 (55%) | 10 (21%) |
| ≤ 405 cells/µL | 46 | 0 | 14 (30%) | 32 (70%) |
| CD3+CD8+ | > 215 cells/µL | 48 | 10 (21%) | 22 (46%) | 16 (33%) |
| ≤ 215 cells/µL | 45 | 1 (2%) | 18 (40%) | 26 (58%) |
| B | > 77 cells/µL | 52 | 8 (16%) | 23 (44%) | 21 (40%) |
| ≤ 77 cells/µL | 41 | 3 (7%) | 17 (42%) | 21 (51%) |
| NK | > 140 cells/µL | 51 | 10 (20%) | 23 (45%) | 18 (35%) |
| ≤ 140 cells/µL | 42 | 1 (2%) | 17 (41%) | 24 (57%) |
{kind=link}
{kind=link}