To the best of our knowledge, this is one of the first studies to examine the relative safety and effectiveness of MP-TSCPC and ECP as adjunct procedures combined with phacoemulsification. Prior studies have mostly demonstrated a limited IOP-lowering effect for phacoemulsification when performed alone. Arthur et al. demonstrated a mean IOP reduction of 2.5 mmHg from a baseline of 16.2 mmHg in a group of 37 patients with open-angle glaucoma.5 Additionally, Poley et al. reported a mean IOP reduction of 2.7 mmHg at 1 year from a baseline of 17.8 mmHg in a group of 124 eyes. The authors noted that the magnitude of IOP reduction was highly correlated with the preoperative IOP.6
The use of combined ECP and phacoemulsification has been well established in the literature.4,7−11 It has emerged as a preferred adjunct microinvasive procedure to phacoemulsification, primarily due to its convenience and low complication rate. Despite its popularity, some data on the long-term effectiveness of phaco/ECP as an IOP-lowering tool has been mixed. In a retrospective cohort study that consisted of 99 POAG patients, Perez et al. demonstrated that the surgical success rate after 1 year was significantly higher in the phaco/ECP group than in the phaco alone group (69.6% versus 40.0%, p = 0.004).12 Similarly, Francis et al. demonstrated mean IOP reductions of 2.7 mmHg and 0.9 mmHg in the phaco/ECP and phaco alone groups, respectively, at 3 years (p = 0.003). Interestingly, the group that underwent cataract extraction alone showed regression to the preoperative IOP after 2–3 years of follow up while the group that received phaco/ECP seemed to maintain the IOP reduction throughout the entire course of the study.13
Other studies have raised into question the ability of phaco/ECP to consistently produce adequate IOP-reduction. In a retrospective study of over 300 eyes, Siegel et al. reported no significant difference in the IOP-lowering effect of phaco/ECP and phaco after 3 years of follow-up. Additionally, Lindfield et al. reported an average IOP reduction of 7.11 mmHg from a baseline of 21.54 mmHg at 18 months, with a mean medication reduction of 0 drops from a baseline of 1.98 drops.9 While the IOP was significantly lowered at each follow-up visit, the authors noted that the reduction was not great enough for phaco/ECP to be considered an alternative for filtration surgery in high-risk eyes, rapidly progressive patients or when a low target pressure (< 14 mmHg) is indicated. With an IOP reduction of 3.07 mmHg in the phaco/ECP group, the reduction at 1 year in the present study was amongst the lowest reported in the literature, despite treating at least 300° of the ciliary processes in all cases. The preoperative medicated IOP here was 15.78 mmHg in the phaco/ECP group, which was amongst the lowest reported in the literature. The comparatively low mean IOP reductions observed here are likely attributable to the low preoperative IOPs, as preoperative IOP has consistently been demonstrated to correlate with the magnitude of IOP reduction.
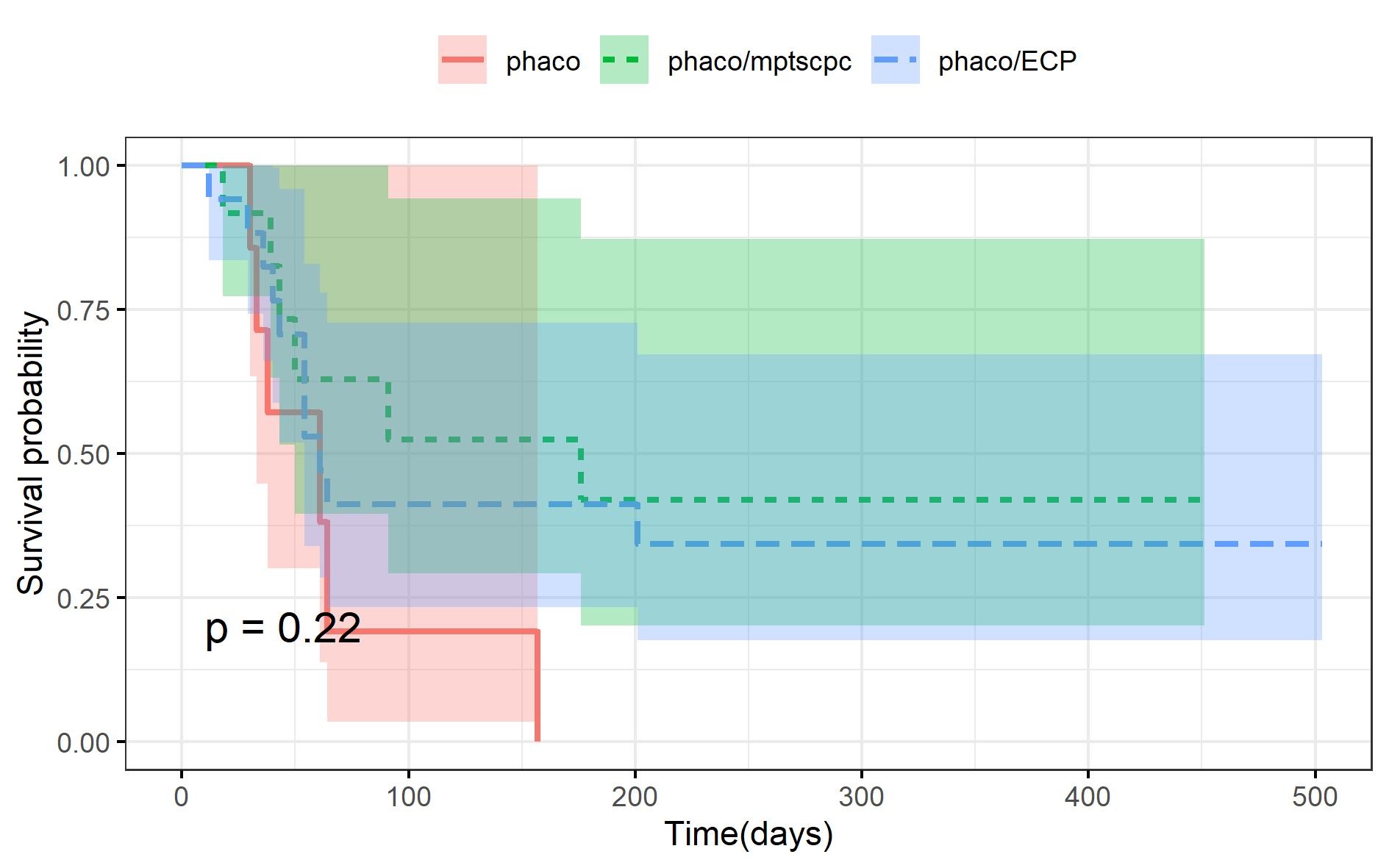
The results of the present study suggest that phaco/MP-TSCPC at least equivalent IOP reduction to phaco/ECP without increasing the risk of postoperative complications. The KM survival curves along with the results of the Cox Proportional Hazards model seem to indicate that phaco/MP-TSCPC may be more effective than phaco/ECP in terms of long-term IOP reduction. The Cox Proportional-Hazards model indicates that phaco/ECP patients were 3.4 times more likely than the phaco/MP-TSCPC group to reach surgical failure at any point in time than the phaco/ECP group. Additionally, it demonstrates that no other pretreatment characteristics, such as type or stage of glaucoma, had a significant effect on the amount of IOP reduction observed. While there was a significant difference in the unadjusted survival curves of the patients who received phaco/MP-TSCPC and phaco/ECP (p = 0.038), this difference only approached significance when the differences in pretreatment characteristics were accounted for (p = 0.052). As with other studies comparing phaco/ECP and phaco, phaco/ECP appeared to provide comparatively greater long-term IOP control than phaco alone. While both the phaco/MP-TSCPC and the phaco/ECP groups outperformed the phaco alone groups in terms of survival rates, combining MP-TSCPC rather than ECP with phacoemulsification seemed to provide for even greater long-term IOP reduction. When the differences in preoperative characteristics were adjusted for, phaco/MP-TSCPC was 3.4 times less likely to reach surgical failure at any time point compared to phaco alone (p = 0.005). The long-term IOP-lowering effect in the phaco/ECP group seemed to be comparatively weaker, as performing phaco/ECP was only 1.4 times less likely than phaco alone to result in surgical failure at any time point (p = 0.038). Notably, the majority of patients included in the phaco/MP-TSCPC group in the present study had severe glaucoma (63%). The use of phaco/MP-TSCPC in this group provided a mean IOP reduction of 6.0 mmHg at 1 year postoperatively, with a mean IOP of 12.37 mmHg at the 1-year visit. Prior studies have demonstrated that the maintenance of IOP within this range is effective in reducing the advancement of visual field defects, particularly in patients with severe glaucoma.14 The sustained IOP reduction observed in this group indicates that phaco/MP-TSCPC may potentially be a useful tool in attaining long-term IOP reduction in severe-glaucoma patients. In the present study, the improvements in visual acuity and reductions in IOP seen in the phaco alone group were less pronounced than in prior studies. The mean preoperative IOP of 14.3 mmHG for the phaco alone group in the present study was amongst the lowest out of all the studies examined. This could potentially account for the seemingly smaller IOP-reducing effect observed, as preoperative IOP was correlated with amount of IOP reduction in the present study as well as in prior studies involving phacoemulsification.5,6 It is important to note that the PH model used in the present study indicated that both the phaco/MP-TSCPC (p = 0.005) and the phaco/ECP groups (p = 0.044) had comparatively greater IOP-lowering effect than the phaco alone group even when the differences in preoperative IOP were considered. The comparatively small improvement in visual acuity is possibly due to the large subset of severe glaucoma patients in this group. It is also possible that the relatively small sample size in this group was insufficiently powered to detect a significant improvement in visual acuity.
In our cohort, post-operative complications were rare and were similar to those reported in the literature. Notably, all cases of postoperative inflammation resolved by the 6-month follow-up visit, and there were no new cases of CME in any group.
This study has several limitations. It is important to note that this study samples patients from a tertiary referral center and we cannot exclude biased referral patterns resulting in sampling bias. In addition, the study’s retrospective design, lack of data on patient adherence, sample size and follow-up duration may also limit generalizability.
In conclusion, the results of the present study indicate that phaco/MP-TSCPC and phaco/ECP may be comparably safe and efficacious in reducing IOP when compared to phacoemulsification alone. Future studies on prospective randomized studies of combined MIGS procedures are needed to elucidate the optimal combination in different patient populations.
{kind=link}