This nationwide, retrospective, longitudinal study aimed to provide a comprehensive review of the age and gender specific incidence and mortality of lung cancer in Hungary, using a novel approach in data collection and study design based on the database of the National Health Insurance Fund of Hungary.
The key findings of this database research covering 6 years can be summarised as follows:
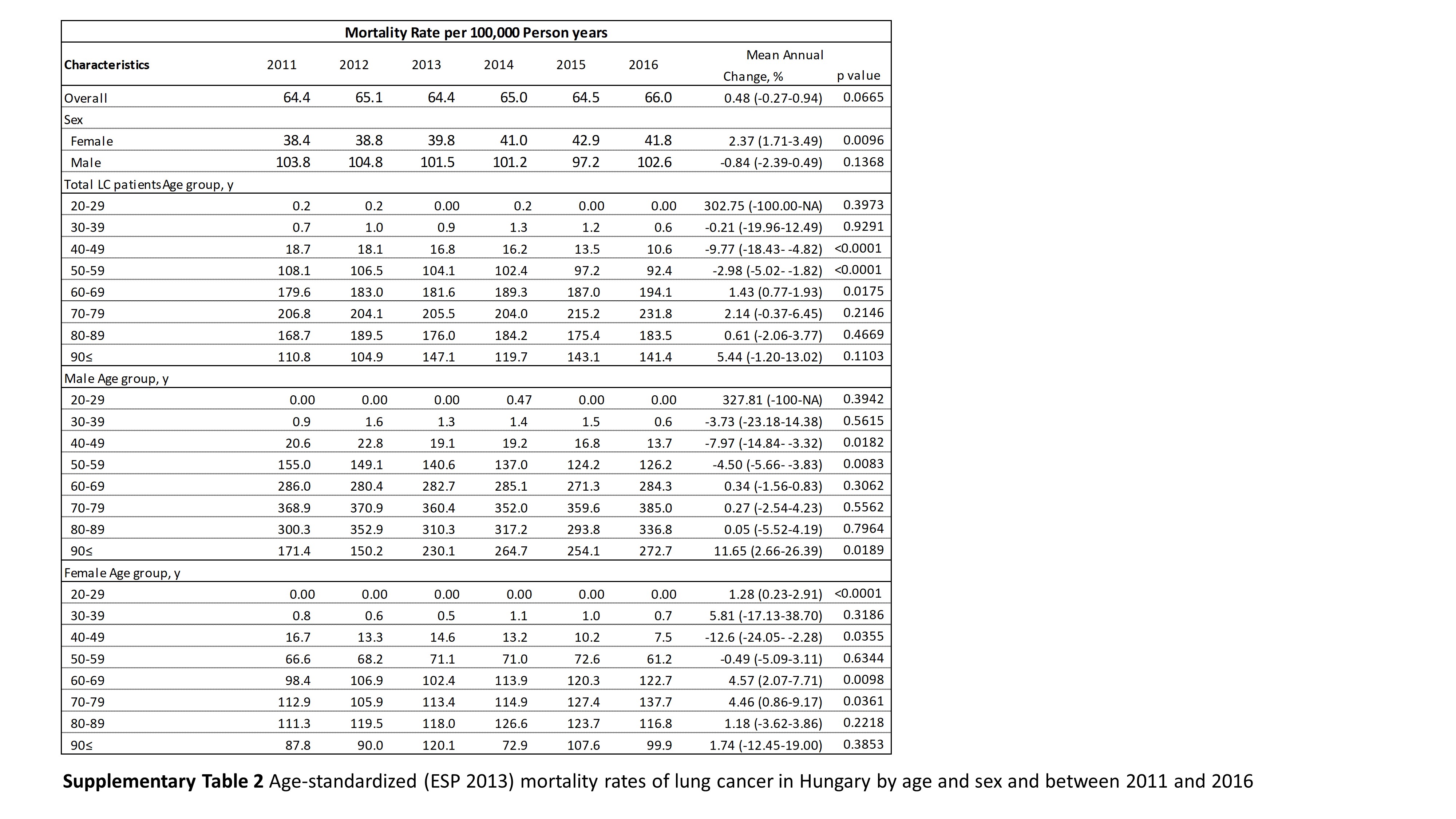
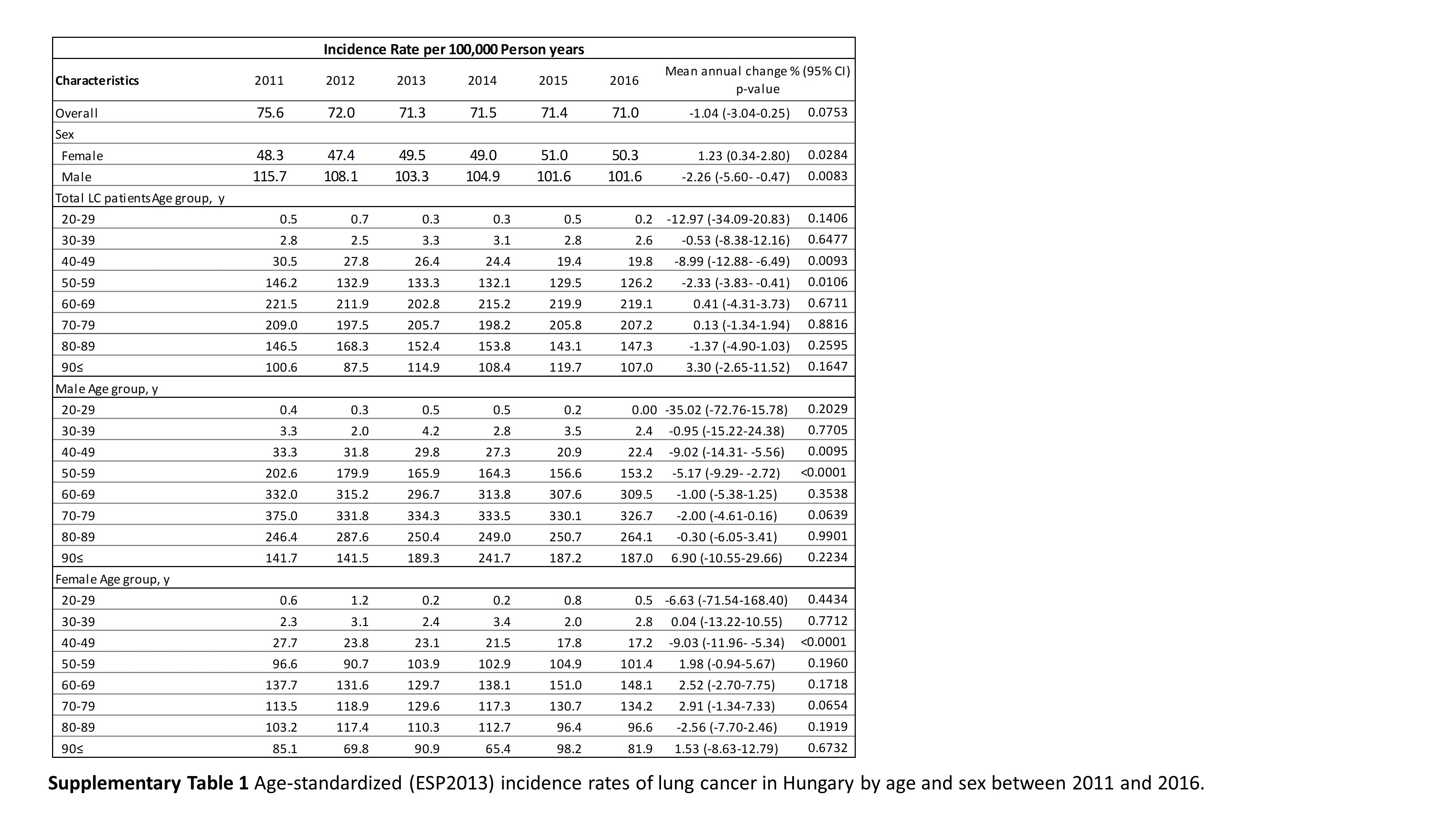
- Age-specific incidence rates of lung cancer were highest in the 70-79 age cohort for men, while it peaked in the 60-69 age group for women.
- While lung cancer incidence rates showed decreasing trends in most age cohorts for men, for females we found an increase in older age groups.
Differences in lung cancer epidemiology based on gender is a quite thoroughly researched topic, showing similar trends across the developed world, with incidence primarily influenced by prevalence of smoking (14,15). Numerous developed countries have reached the peak of their respective tobacco-related lung cancer disease burden, thus incidence and mortality rates started to decline, exhibiting major differences by gender. Historically smoking was always more prevalent among men, leading to higher rates of lung cancer incidence and mortality worldwide (16,17). Women took up smoking at a later period, mostly after the Second World War, and their rates of cessation have lagged behind those of men, leading to a much later peak in lung cancer incidence (18). In the United States age-standardized incidence rates for males have declined from a peak of 102 in 1984 to 69/100,000 PSYs by 2009, displaying a strong correlation with the decline in smoking prevalence since the 1980’s (18,19). However the trend is showing an opposite curve for females, with age-standardized rates reaching 51/100,000 PSYs, a major increase since 1984, from 39/100,000 PSYs (20).
Similar trends were found in our recently published nationwide NHIF database study where incidence rates among men declined significantly from 115.7 to 101.6 per 100,000 PSYs during the 6 year study period, equivalent to a decrease of 2.35 percent (12). This trend mirrors the decreasing smoking prevalence rates among Hungarian men, declining from 44% in 1994 to 31% in 2014 (21). In the current analysis, the highest, 11% reduction of male lung cancer incidence was found in the age group of 40–49 years, although a less pronounced but still significant 4% change was detected in the age group of 50–59 years. In our study, the decrease in the incidence of lung cancer was not significant in older male cohorts (above 60 years), which can probably be attributed to the shorter observation period and relatively low patient numbers. Nevertheless, the significant decrease in middle-aged male population may reflect the efficacy of antismoking initiatives in Hungary in the last decades (22). On the other hand, we found increasing rates of lung cancer incidence in the whole female study population, with an annual increase of 2.37%. However, detailed age dependent analysis shows mixed results, the increase was significant in older age groups, while a decrease was detected in the age group of 40–49 years. These findings correspond to a study by Thomas et al. that compared the incidence of non-small cell lung cancer (NSCLC) in lung cancer patients younger and older than 40 years and found decreasing trends between 1975 and 2010 in both cohorts of males, however opposite trends in females lung cancer population, where younger patients had already decreasing trend on incidence, while older(40<) had still increase in incidence rate (23). Akhtar-Danesh et al. also reported a decrease in the incidence of lung cancer among women in the age group of 50–59 years, and an increase over the age of 60 (24).
Differences in incidence of lung cancer among the genders could be explained by several factors (26), however, it can be concluded that the most important risk factor for the development of lung cancer is smoking in both genders (26). Smoking among women has significantly increased since the 1960s, resulting in a consequent increase in the risk of death in the female population(27). The window of our study most probably covers a period, when we could capture the impact of changing smoking habits due to impact of anti-smoking campaign and initiatives (22). The European Health Interview Surveys reported smoking prevalence data from Hungary. In 2000, the smoking prevalens of males 18–34, 35–64, 65≤ age cohorts were 44.4%, 41.1% and 13.7% respectively, while similar rates in 2009 was 36.3% and 36.4% in 18–34 and 35–64 age groups, and 14.1% in the oldest one, showing a 18.2 and 11.2% decrease for the two younger cohorts. On the other hand, we could find a 11.7% decrease at females only in the 18-34 age group (29.0% onto 25.6% during 2000-2009 period), but plateauing trend was seen in the older female population (28.2% to 28.8% and 3.4 to 7.0%) (28). In their latest report describing smoking habits in Hungary they reported that smoking prevalence have almost equalized among the genders: the proportion of male smokers showing a steady reduction (32–34%), with the prevalence of smoking stabilizing at 24–25% of the population (29). This shifting prevalence of smoking is also in line with our findings showing a diminishing difference in the risk of lung cancer incidence and mortality between the genders in all age cohorts. The decreasing smoking prevalence at all male age cohort in the 2000s years could be reflected in the decrease of lung cancer incidence in the 2010s, while the peaking smoking prevalence at females are reflected in the increasing lung cancer incidence at most age groups of our study population. The increasing incidence of adenocarcinoma among non-smoking women may also play a role in the narrowing gap between males and females (30). Introduction of a comprehensive and rigorously enforced anti-smoking laws of 2011 and 2013, the reduction in retail tobacco selling points, the new multi-media awareness campaign focusing on young generations and the foundation of a Methodological Support Centre for Smoking Cessation at the National Korányi Institute of Pulmonology may have further positive effects in the future by improving lung cancer trends in upcoming decades, in both sexes.
It is observed that the incidence of lung cancer shows strong correlation with age: rates usually start to increase from the age group of 45–49 years, with the highest rates observed in the 85–89 age group among men and in the 80–84 age group among women (31,32). In the UK Cancer Research database, we found similar result: male incidence peaked in 80 or above age cohort close to 600 per 100,000 PSYs, while the rate did not exceed the 100 per 100,000 PSYs till the age of 50 (33). The peak of incidence was also found in the age group of 80–85 years in the United States as reported by Lung Cancer Statistics, while the highest rate among women was found in the 75–80 age group (34). The Hungarian male age specific lung cancer incidence rate sharply increases from 40 to 49, exceeding 100 per 100.000 PSYs already by the 50 to 59 age cohorts, peaking in the 60 to 79 age groups, then sharply decreases at 80≤ age groups in both genders. This result is partly different from UK and US trends where the peak of incidence was found in older age groups. The UK Cancer Research database(4) gives detailed tobacco smoking prevalence information, indicating lower smoking prevalence in the younger male and female age groups compared to Hungary but no relevant differences could be found in the older age groups. We could find similar differences in the age specific mortality rates. The earlier peak in the Hungarian lung cancer incidence could be explained by the higher smoking rates, however the lower incidence and mortality rates above the 80 age cohort could be explained by the higher cardiovascular risk of Hungarian population, (35) acting as a competing morbidity, resulting in earlier mortality especially among regular heavy smokers (36).
There are certain strengths and limitations of our study. The coverage of the whole population in the NHIF database to identify lung cancer patients, the carefully cleaned data, the 6-year-long follow-up period, all provide a solid foundation for drawing conclusions from our analysis. Nevertheless, NHIF database does not contain any data on the staging or the Eastern Cooperative Oncology Group (ECOG) Scale of Performance Status of patients, and no laboratory test results were available. Besides, we were not able to examine the competing cause of death in the lung cancer population.

{kind=link}
{kind=link}