HMGB1 is a highly conserved non-histone nuclear protein that is abundantly expressed in most eukaryotic cells (106 molecules/cell). Composed of 215 amino acids, HMGB1 in the nucleus can regulate the stability of nucleosomes, participate in the recombination, replication, repair, and transcription of DNA, and can be actively or passively released under physiological and pathological conditions to exert an inflammatory cytokine-like role. In the nucleus, the HMGB1 protein generally binds to the minor groove of the DNA double helix on the nucleosome, and the nucleosome and its components, such as nucleosomes, histones, DNA, etc., are a large source of autoantigens(9, 10). Based on these, it is inferred that HMGB1 may also cause an autoimmune response, produce autoantibodies, and cause autoimmune diseases. A large number of studies, including our previous basic work, have shown that HMGB1 plays a role in the occurrence and development of infectious diseases and autoimmune diseases. It, therefore, is an important point in the regulation of immune homeostasis, which may be an important target for the diagnosis and treatment of related diseases.
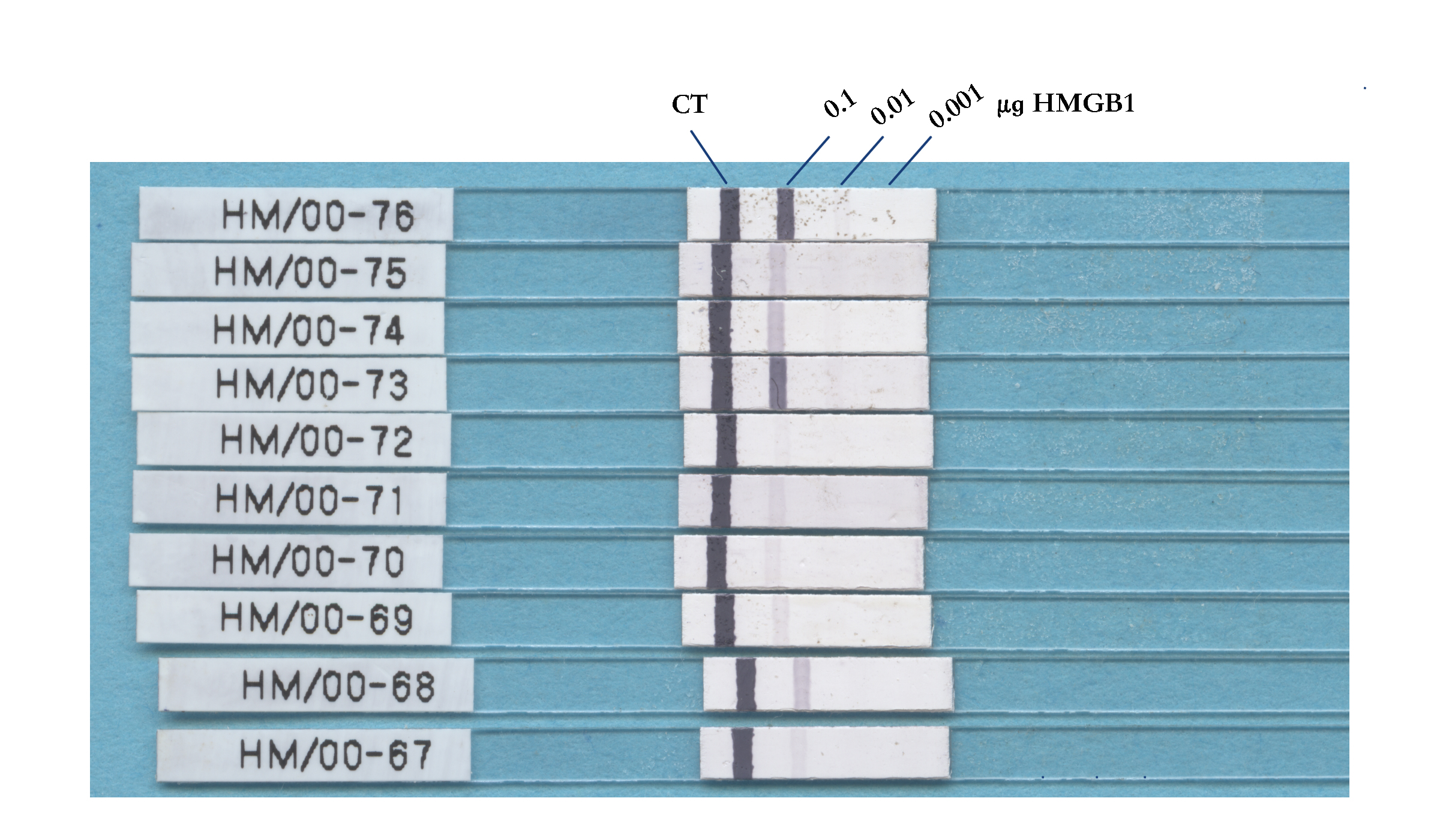
Laboratory indicators play a key role in the diagnosis and efficacy monitoring of autoimmune diseases. Indirect fluorescent ANA screening and detection of related autoantibodies can provide important evidences for the diagnosis and differential diagnosis of autoimmune diseases(1). In SS, ANA shows a typical granular fluorescence pattern. The presence of multiple autoantibodies in patients with SS is one of the characteristics of the disease. Among these patients, anti-SS-A autoantibody can be detected in about 70% of the patients, and SS-B autoantibody can be detected in 45% of the patients. In some ANA-positive patients, both anti-SS-A and SS-B antibodies are negative, indicating that there are some autoantibodies with other characteristic in SS patients. Through in-house built ELISA and immunoblotting, we found that the serum anti-HMGB1 antibody level in SS patients increased. Taking 8 RU/ml as the cut-off value, the sensitivity and specificity of diagnosing SS reached 64.5% and96.9%, respectively, and the area under the ROC curve was 0.83, which had potential clinical application value.
The nuclear components are abnormally recognized by the body's immune system and produce autoantibodies, which is an important pathogenesis of autoimmune diseases. Whether HMGB1, as a non-histone nuclear protein, can cause the body's autoimmune response and lead to pathological changes is one of the hotspots of research. Many studies have shown that anti-HMGB1 antibodies can be detected in patients with systemic lupus erythematosus (SLE) (8, 11–13), and it is related to the severity of the disease. A variety of autoantibodies can appear in patients with autoimmune diseases, which have certain disease specificities, such as anti-ds-DNA antibodies and anti-Sm antibodies in SLE patients. There are also some antibodies that can be presented in multiple autoimmune diseases, for example, anti-ss-DNA (single-stranded DNA) antibodies can be detected in SLE, mixed connective tissue disease (MCTD), and polymyositis/dermatomyositis.
In this study, it was found through immunoblotting detection that 61 (70.1%) of 87 patients with ANA-IF exhibiting a typical granular fluorescence pattern were positive for anti-HMGB1, among whom 43 patients (49.4%) were positive for anti-SS-A, and 20.7% (18) were positive for anti-HMGB1 alone, suggesting that anti-HMGB1 antibody was one of the sources of fluorescence in the ANA-IF experiment. Then commercial anti-HMGB1 antibody was used to study the typical fluorescence pattern of anti-HMGB1 antibody. Fixed Hep-2 and monkey liver slices were used as the matrix, and the anti-HMGB1 antibody presented a typical granular fluorescence pattern, which was consistent with our hypothesis. Some studies have shown that the anti-HMGB1 antibody presented a diffuse cytoplasmic staining pattern, which is believed to be caused by activation of tumor cells, and then HMGB1 exits the nucleus and enters the cytoplasm(12). Our experimental results showed that the fluorescence pattern of anti-HMGB1 antibody in HEP-2 showed a typical granular pattern, and the fluorescence in the cytoplasm was very weak. The fluorescence in the monkey liver slices also showed a granular pattern. Taking the fact that HMGB1 is a nuclear protein into consider, we believe that granular fluorescence pattern is the actual pattern for anti-HMGB1 antibody.
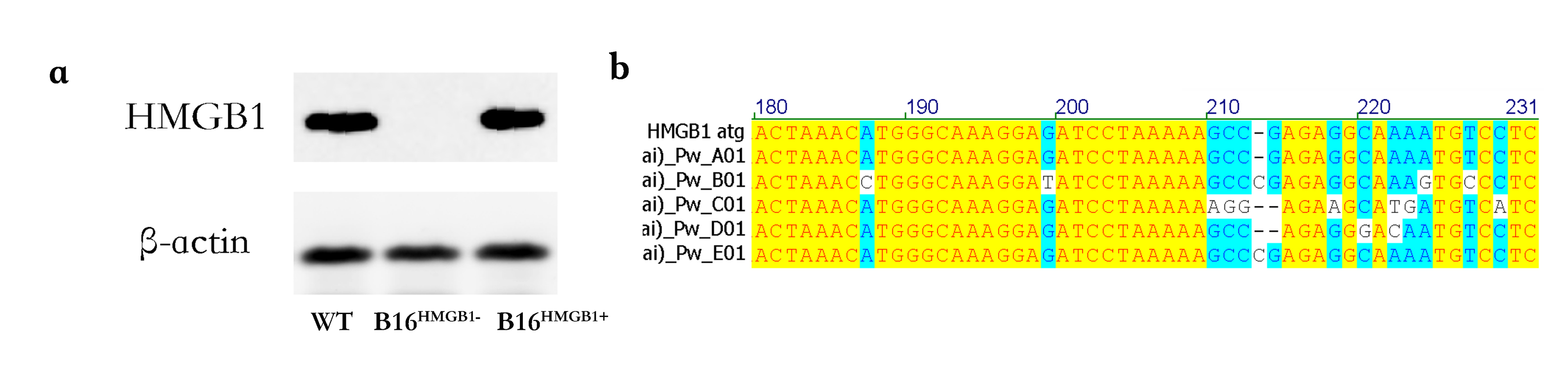
In order to further confirm that anti-HMGB1 antibody is one of the characteristic autoantibodies of SS, we used Cas9 technique to construct a HMGB1 knockout mouse melanoma cell line B16HMGB1− to repeat the ANA-IF experiment. The results showed that ANA (+ or ±), SS-A (-), and SS-B (-) serums showed typical granular fluorescence pattern in wild-type B16, but there was no fluorescence in B16HMGB1−, confirming that ANA-IF fluorescence came from the anti-HMGB1 autoantibodies in the patients.
In conclusion, the results of this study show that anti-HMGB1 antibody may be one of the characteristic autoantibodies of SS. The detection of anti-HMGB1 antibody can provide laboratory evidence for clinical diagnosis of SS, and further improve the accuracy of SS diagnosis based on the existing detection indicators. Further research on the role of HMGB1 in the pathogenesis of SS may lead to the development of new drugs or treatment strategies for the treatment of SS.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}