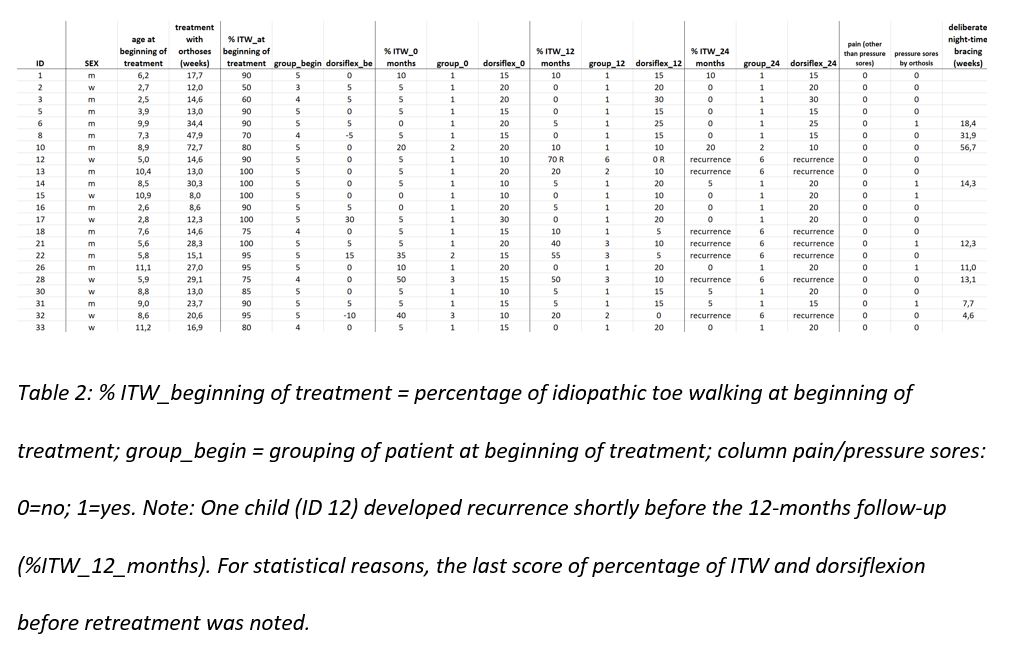
12 months after the treatment with the lower leg orthoses with a circular foot-unit following the Baise/Pohlig design, 73% of our patients (16 of 22) showed no or just sporadic idiopathic toe walking (less than 10% of time spent walking). After 24 months, 64% of the patients (14 of 22) had a normal walking gait.
These results are quite favourable compared to previously published ones. In 2013 Engström et al. provided 51 idiopathic toe walkers with a lower leg cast for four weeks and additionally randomized 21 patients to botulinum toxin injections into the calf muscles beforehand. After twelve months, only 12% (cast) and 30% (cast + botulinum toxin) of their patients showed a normalized gait pattern in parents’ perception [10]. Sätila et al. (2016) treated 30 children with stretching exercises for one-year, indoor shoes with solid heel caps and night-time splints made of a softcast, which had to be worn at least five nights a week. 16 of these patients received botulinum toxin injections into the calf muscles additionally. After 12 months, 28% (conservative group) and 56% (cons. + botulinum toxin) walked normally, after 24 months 54% and 50%, respectively [8]. Only Jack et al. were successful by completely seizing toe walking in all of their 10 children observed after 12 months using a combination of botulinum toxin, 1-3 weeks of walking cast and night-time bracing[11].
Surgical interventions to correct muscular shortening have been investigated with heterogenous results. Eastwood et al. showed that only 22% of surgically treated patients (Baker type of aponeurotic lengthening of the Achilles tendon; 10/46) showed a normal gait after 7.9 years (range 2-22). McMulkin et al. 2016 showed that after surgical lengthening of the gastrocnemius/soleus muscle after five years six out of eight patients had a normalized gait pattern [2].
To date, classical AFOs could not be proven to provide proper treatment of ITW so far[14]. Herrin et al. investigated the effect of classical AFOs compared to carbon insoles in a cohort of 18 patients (figure 7) [7]. Parents did not find an improvement in their walking pattern after six weeks
We are convinced, that the ring-type design of the orthosis subject of our investigation is well capable of correcting the position of the foot and in this situation especially of the talocalcaneal complex regarding to the tibia. With the widely-used classical ankle foot orthosis (AFO), being a dorsal half-pipe with Velcro-straps at the foot and lower leg (figure 5-A), we did observe that the heel and the hindfoot can move inadequately in an equinus situation within the orthosis, especially while walking. In 2005 on the other hand Baise and Pohlig demonstrated for the first time in 260 patients suffering cerebral palsy that an equinus position can be corrected in 84% using a lower leg orthosis with a circular foot unit [15]. In a previous study with paediatric clubfoot patients our research group showed that the orthosis is capable of controlling the foot in all three planes [12]. The position of the foot in the orthosis cannot or merely be altered by evasive movements, like being held in a cast.
According to the Cochrane Paper by Caserta and Williams (2019), orthotic treatment of ITW patients should facilitate better ankle movement. It should include walking treatment, modulation of sensory processing or enhancement of motor control [9].
Ankle mobility does improve with muscular stretching of both the soleus and the gastrocnemius muscles. The single articulated soleus muscle is stretched during the pre-swing phase of the walking cycle, when the foot is brought into dorsiflexion (possible in our orthosis because of the hinges). Furthermore, knee extension will stretch the double articulated gastrocnemius muscle in mid stance (facilitated in our orthosis by prevention of plantarflexion).
Previous groups have shown, that cast treatments can normalize toe walking gait patterns for a few weeks[19, 20]. Because our orthosis works similar like a walking cast, we assumed that the impact on the motor control should be comparable. The use of the orthosis while walking could thus possibly restructure the walking pattern and improve dyspraxia[16-18].
Deliberate night-time bracing was continued in our study group by 41% of the patients for an average of 19 weeks and seemed to have a positive influence on the gait pattern during daytime. This might be explained by the sensory processing modulation taking place via stimulation of proprioceptive and tactile receptors during subconscious movements while sleeping. A dysfunction of sensory processing has been associated with ITW in multiple studies in the past [21-25]. Williams et al. (2014) found a connection between partial dysfunction and hyposensitivity to tactile stimuli due to an immature or mild impaired cerebellum or motor cortex in ITW [26]. Consequently, we added a toe elevation plate from the second to the fourth toe to enhance stimulation of the tendon receptors by enhancing pretension of the flexor tendons.
The assumption exists that younger children may benefit more from serial casting [27]. Contrary to previous results, older patients suffered less recurrences than younger ones in our small group of 22 patients.
We decided to choose the parents’ perception of ITW as a primary outcome parameter. Because children tend to show their “best walking” under examination and intentionally suppress the toe walking in the gait laboratory or when feeling observed. Both would confound objective examinations. Other groups reported similar observations [7, 8]. This point of view is not shared by all groups examining ITW [28]. Smart wearables, for example insoles or socks with pressure receptors could be useful additions in future studies.
We are cautious to combine orthotic treatment with botulinum toxin. We do not think that the literature does sufficiently prove advantages of this measure [10, 18].
Limitations of the study
Retrospective observations could be confounded in general. The information value of our study is limited by the small number of cases and the absence of a control group.
{kind=link}