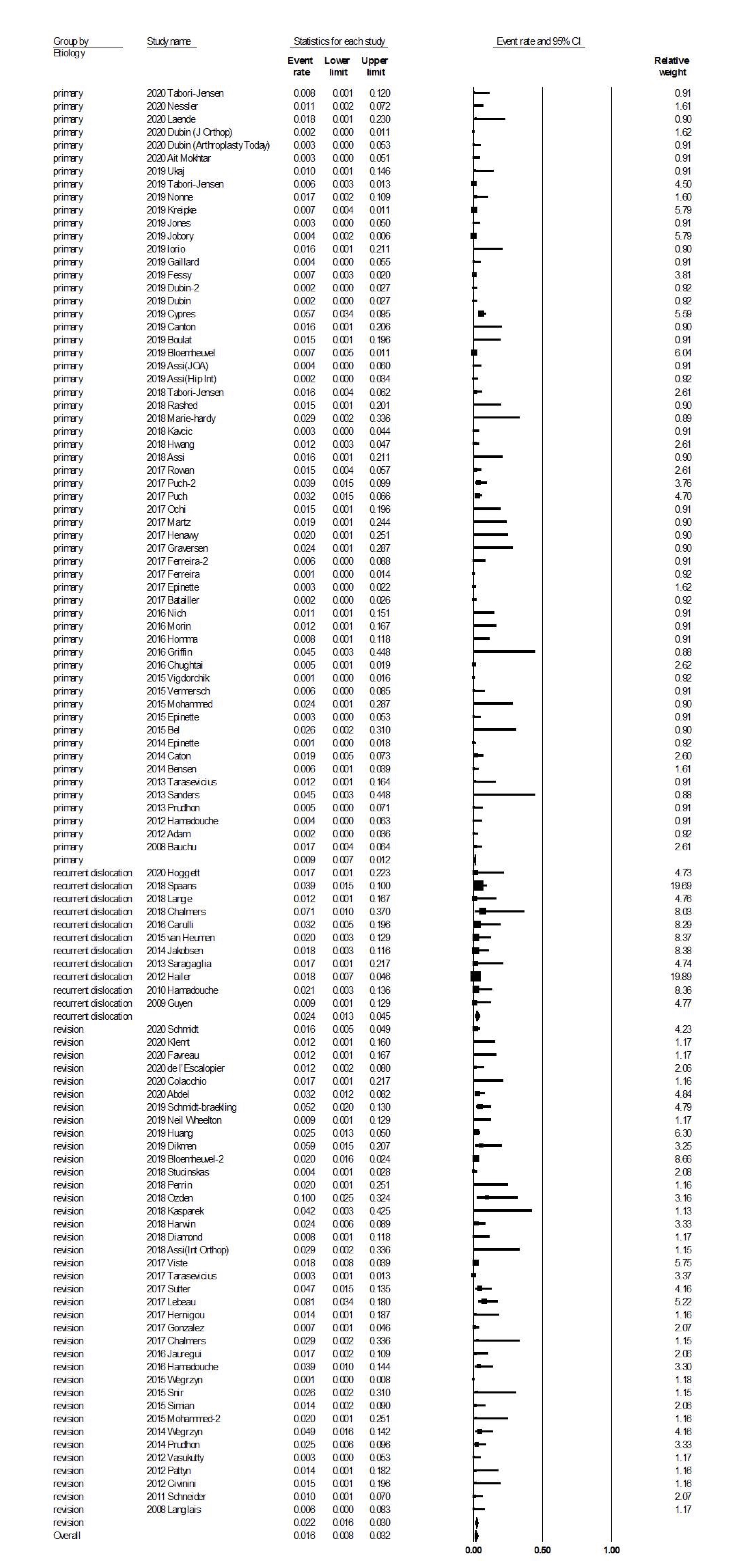
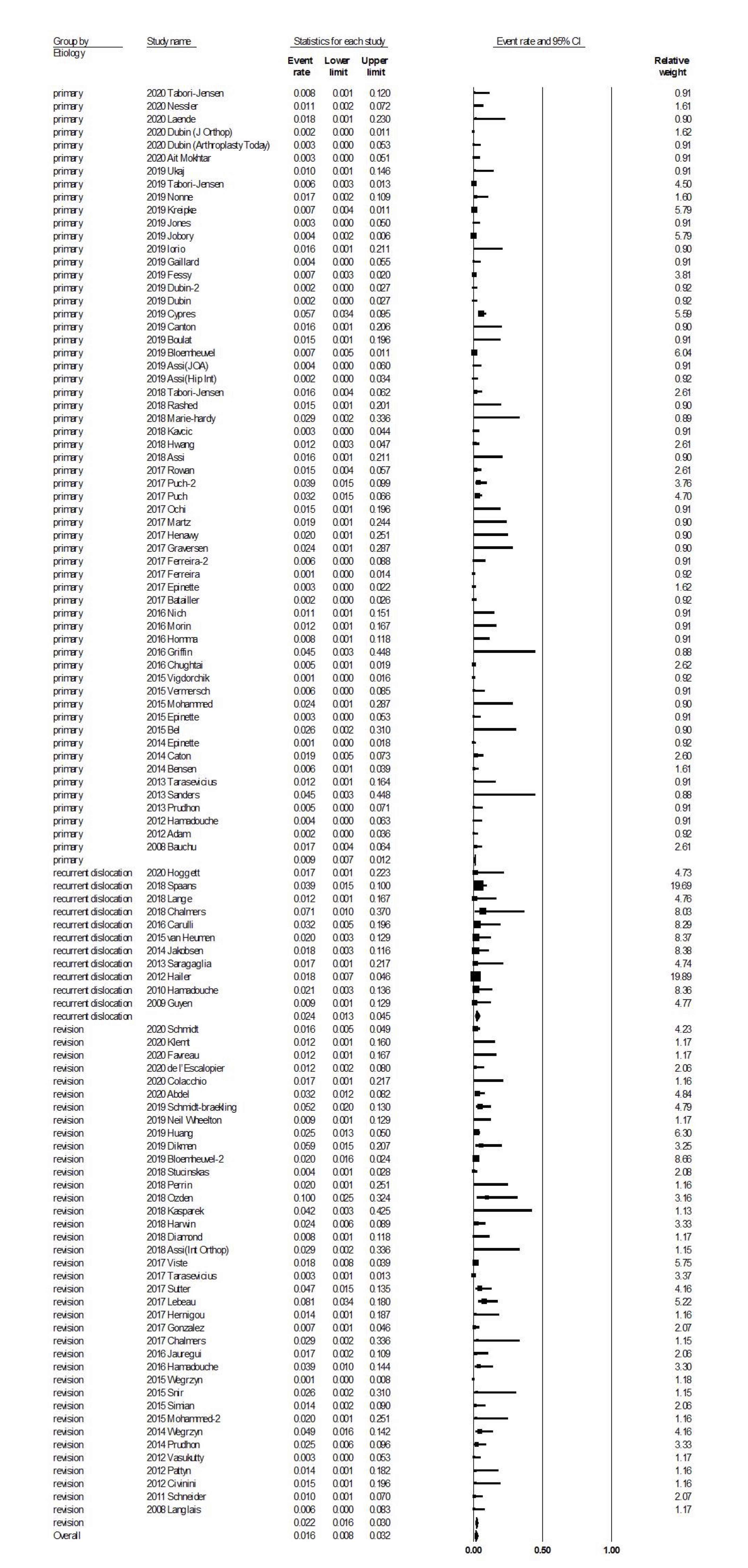
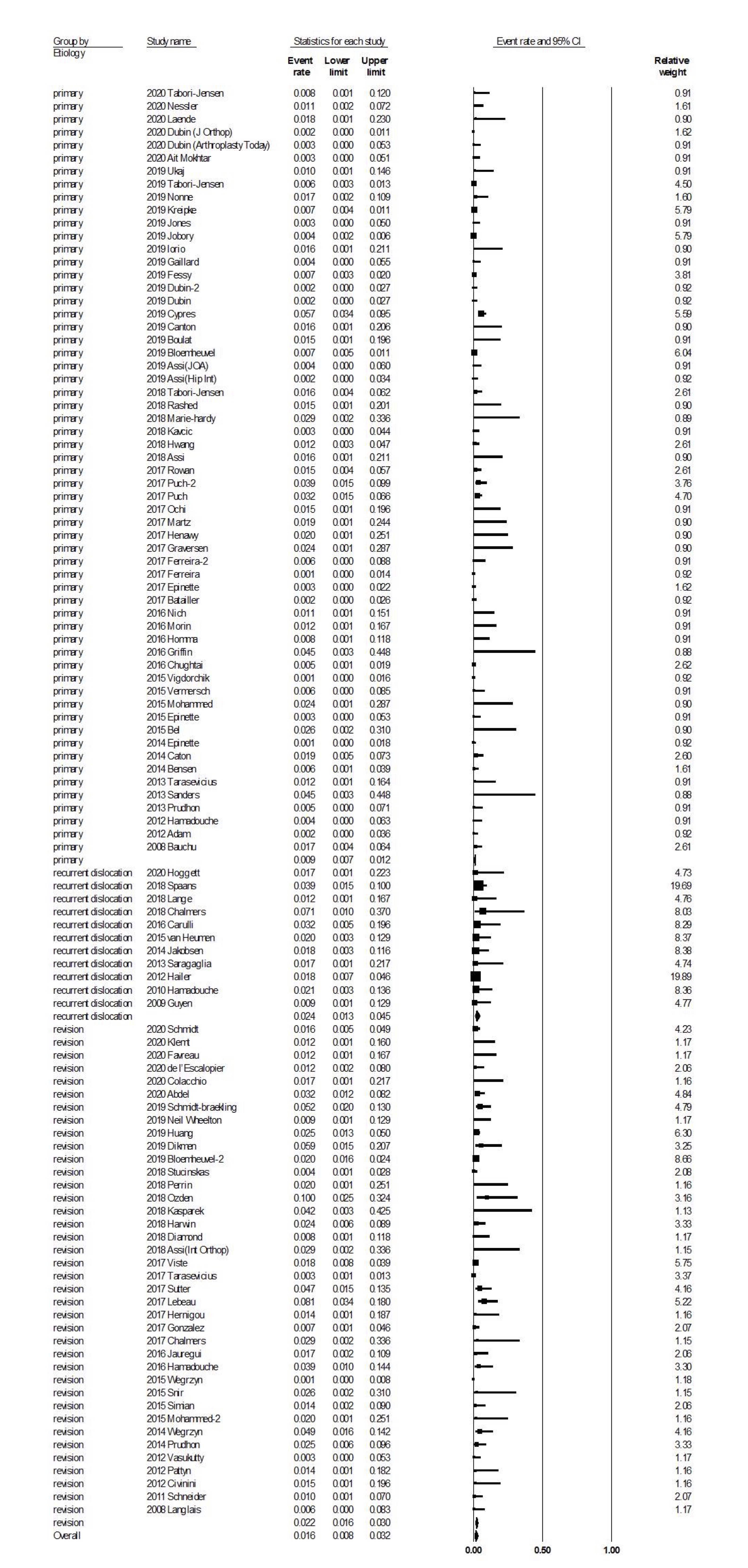
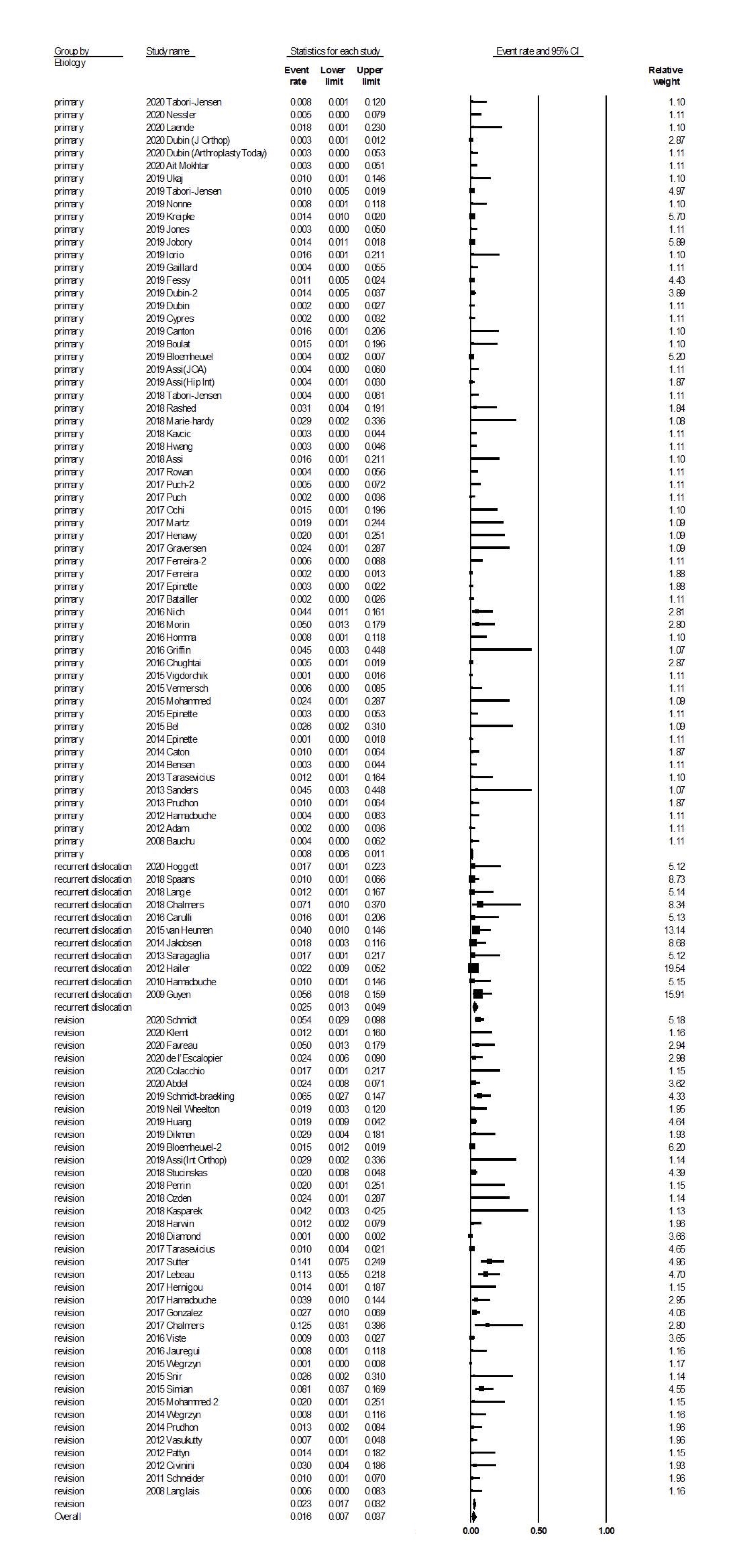
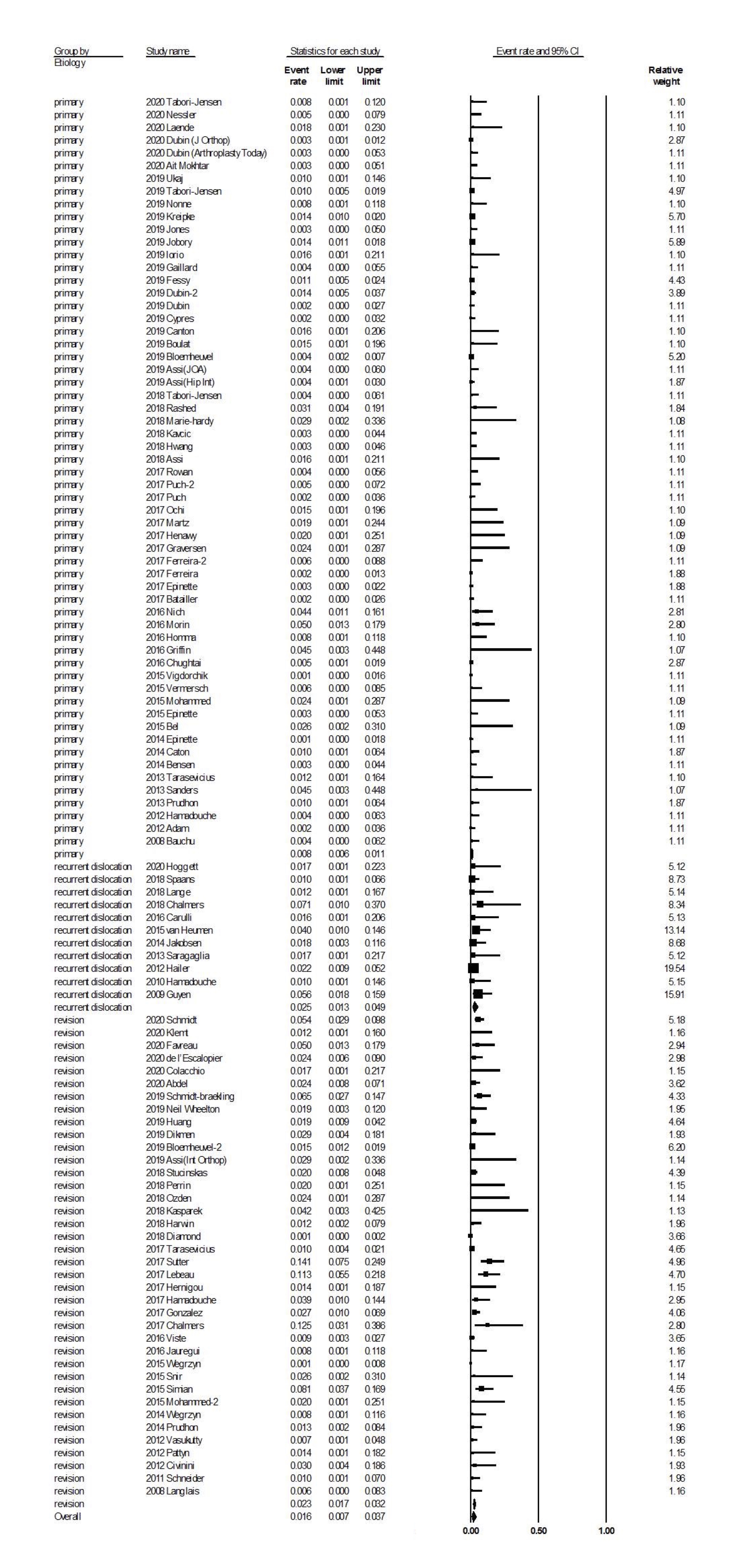
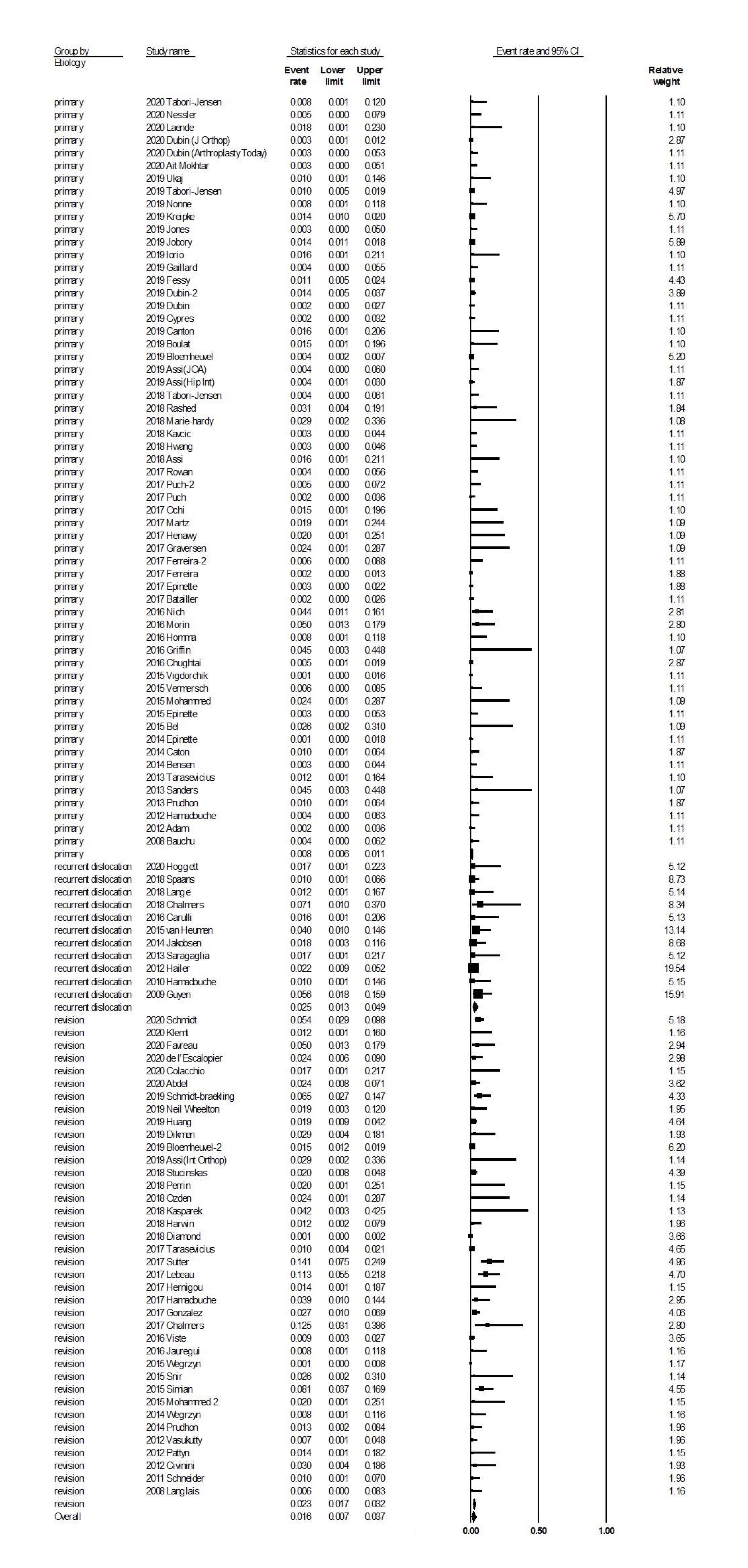
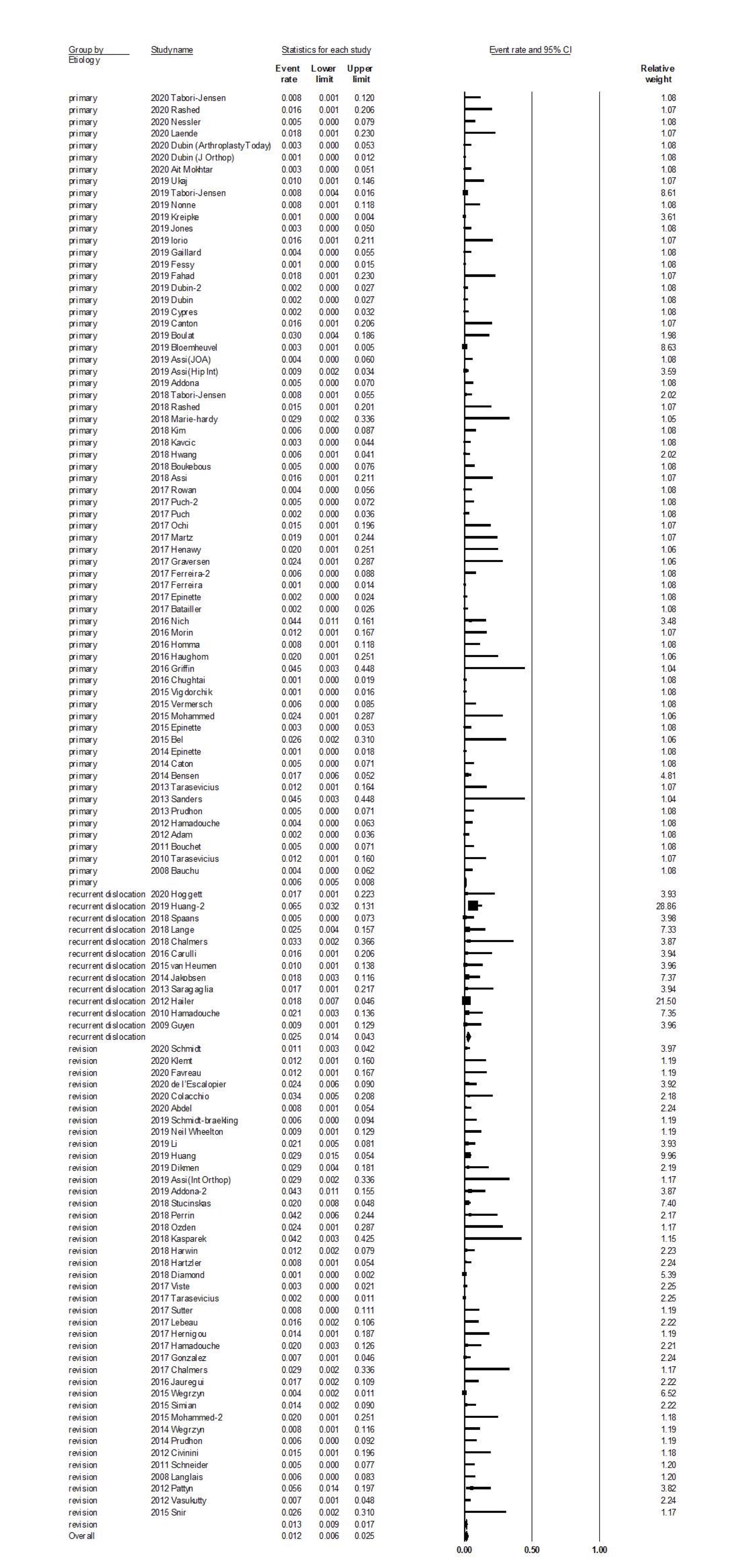
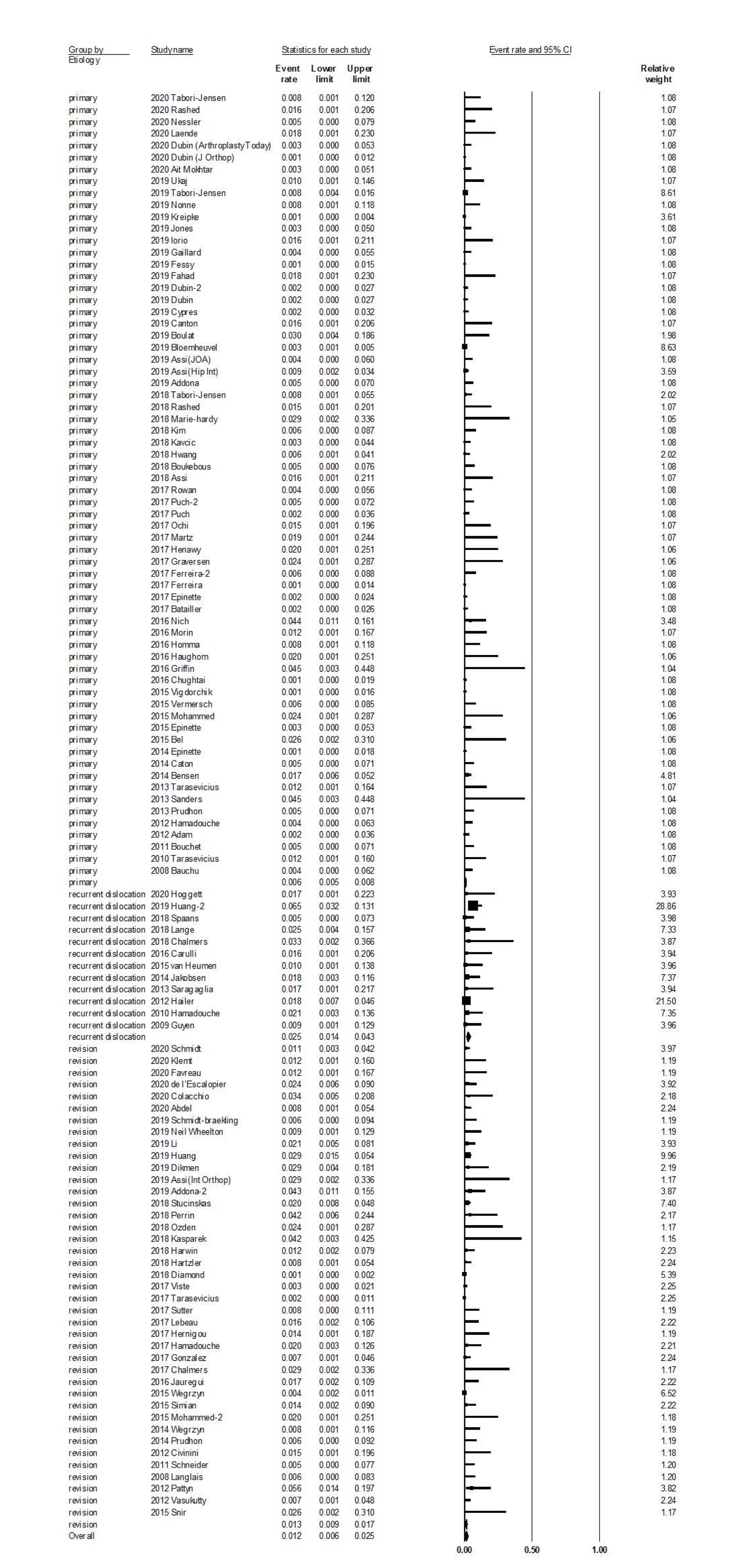
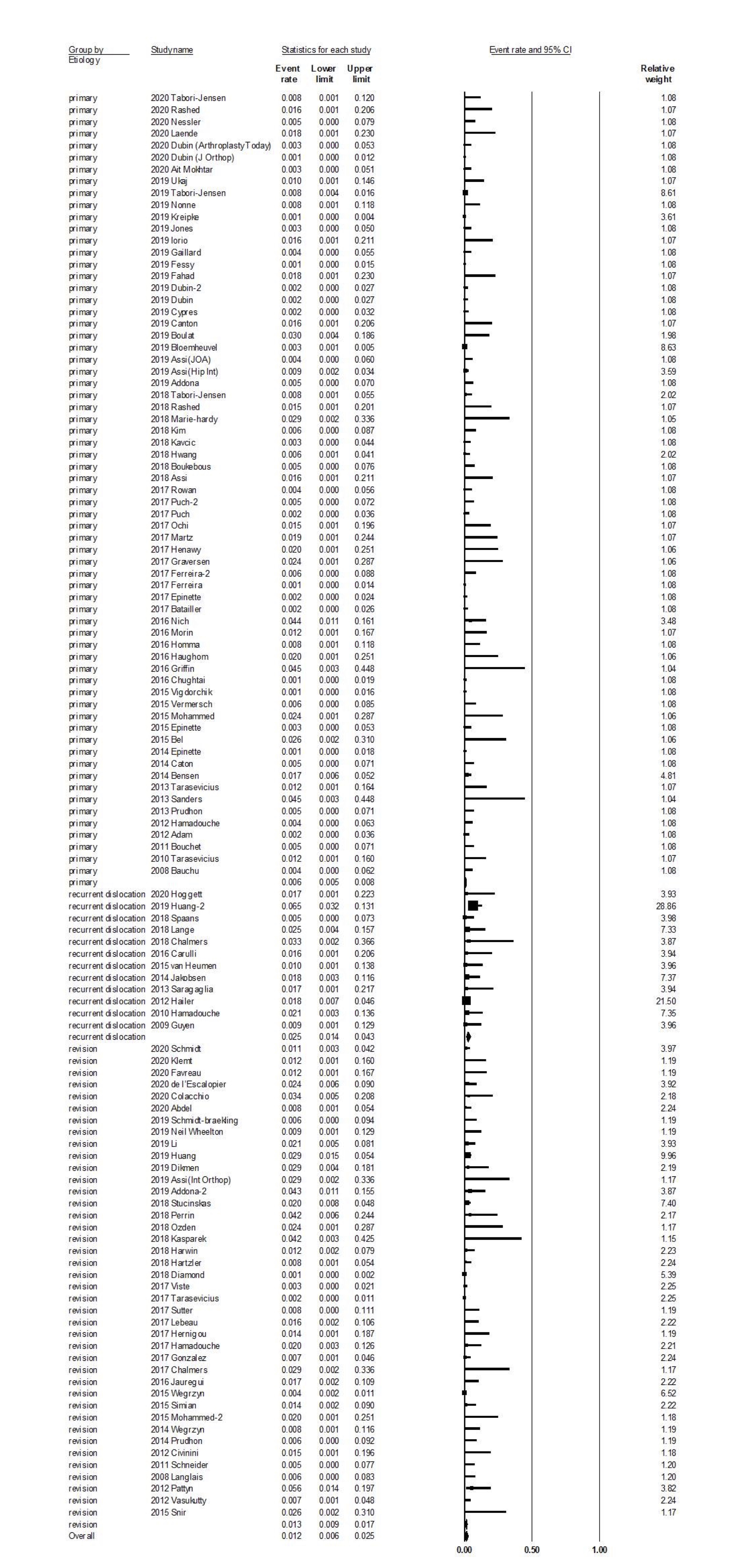
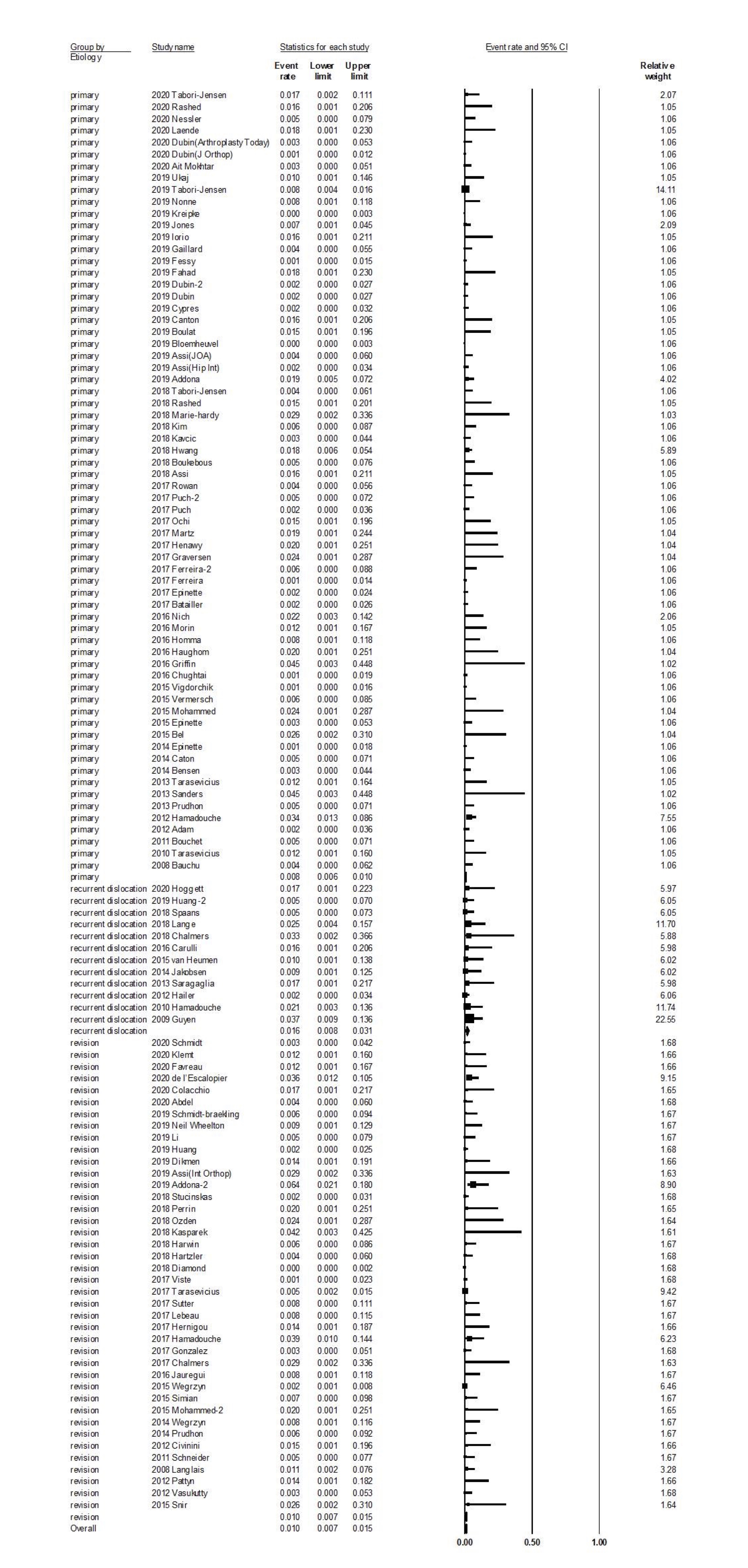
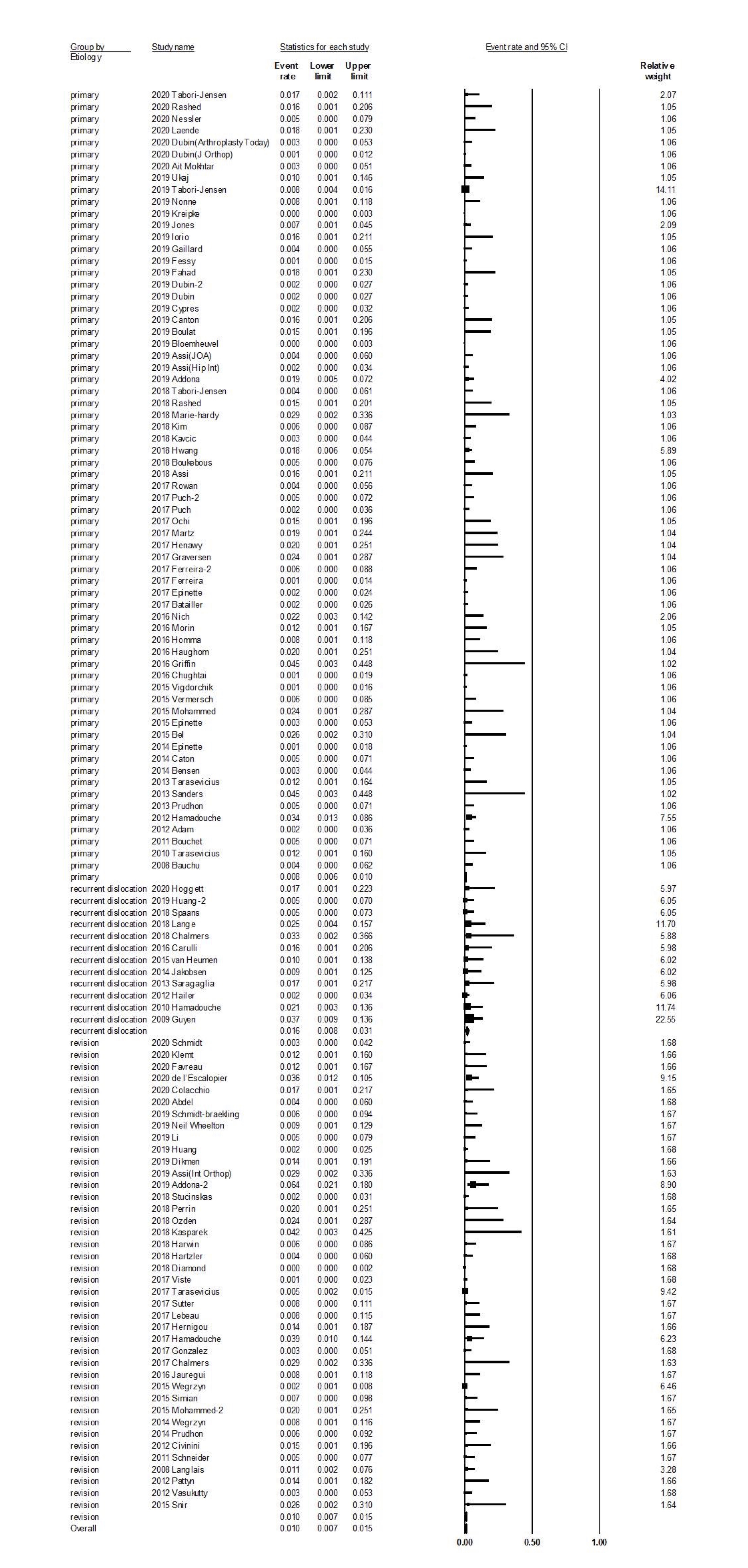
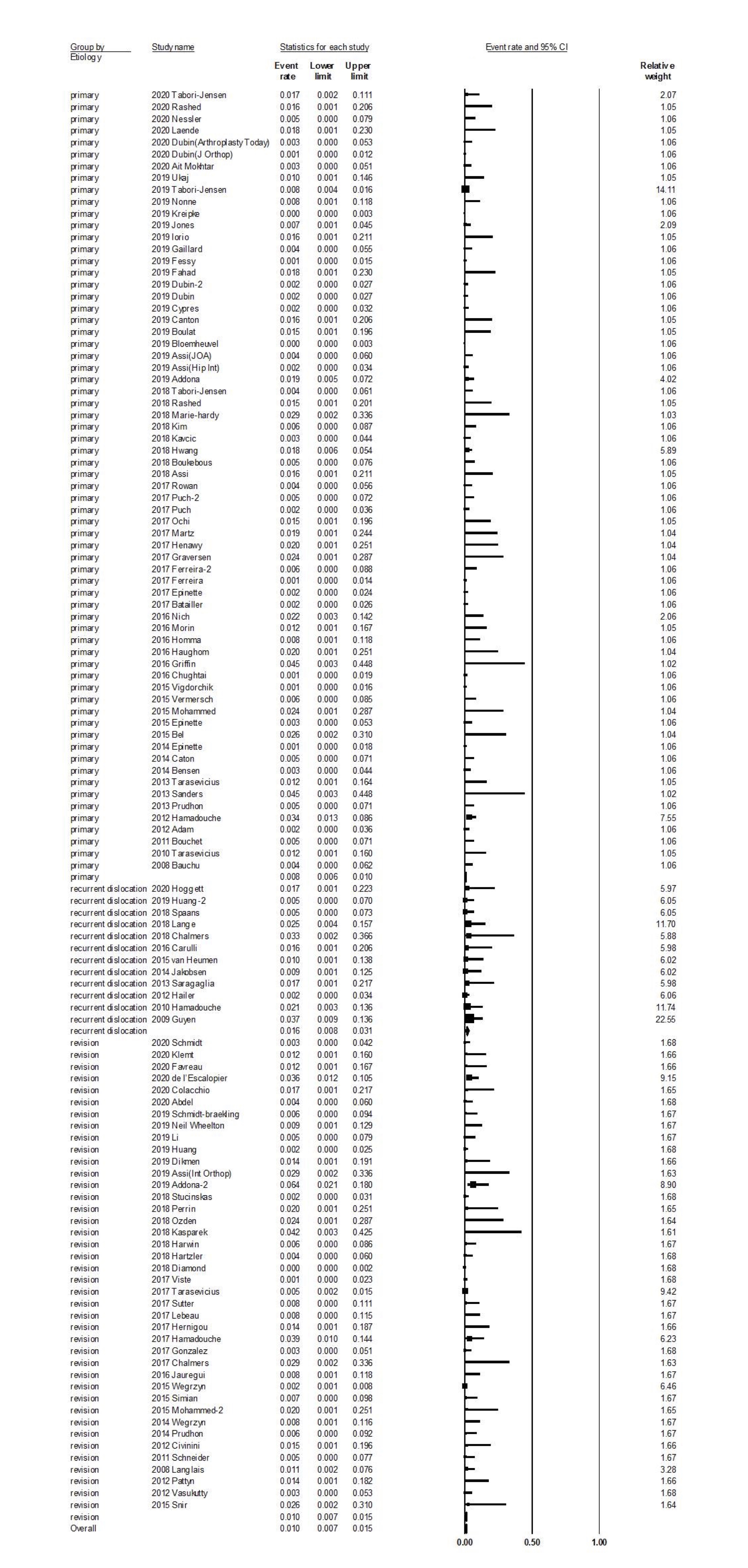
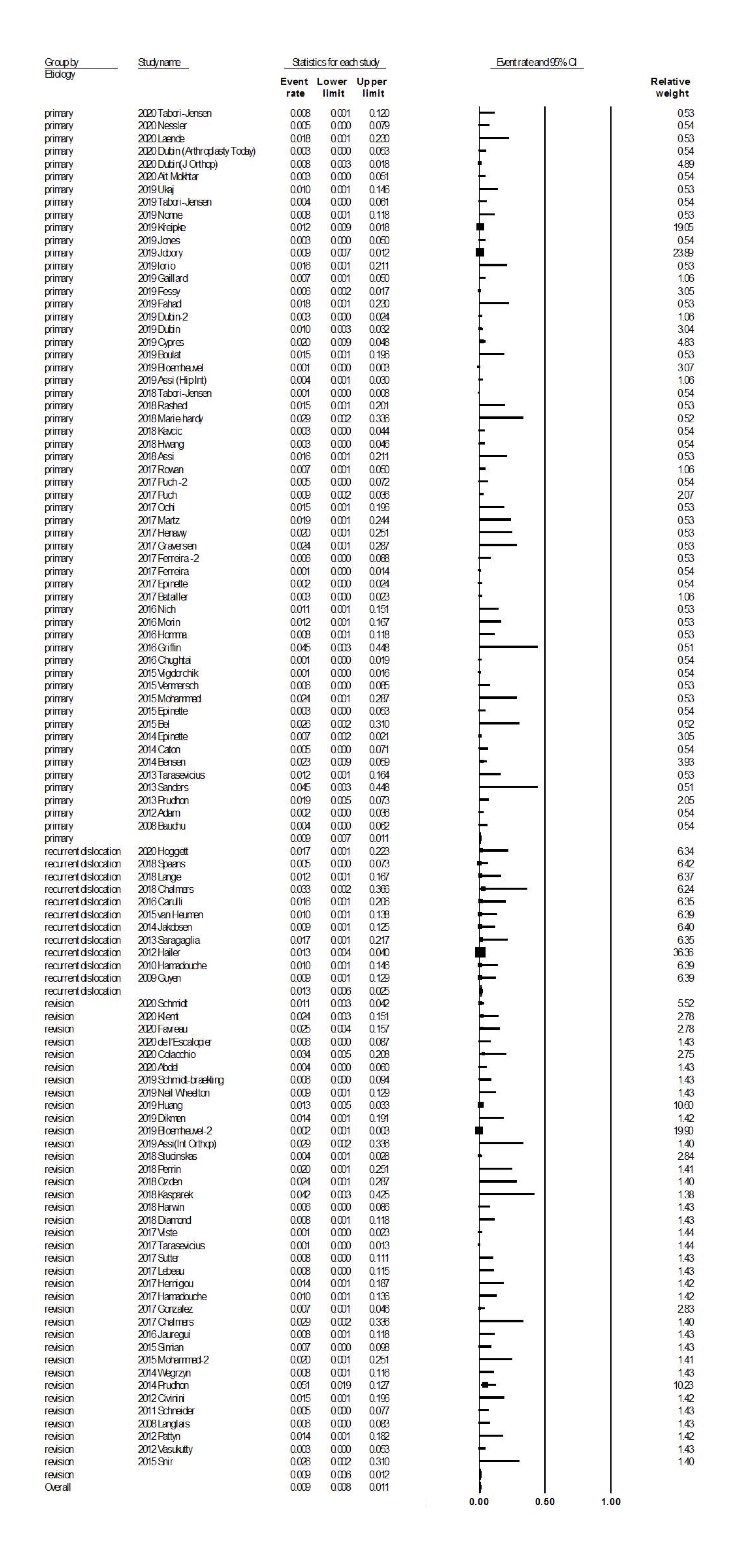
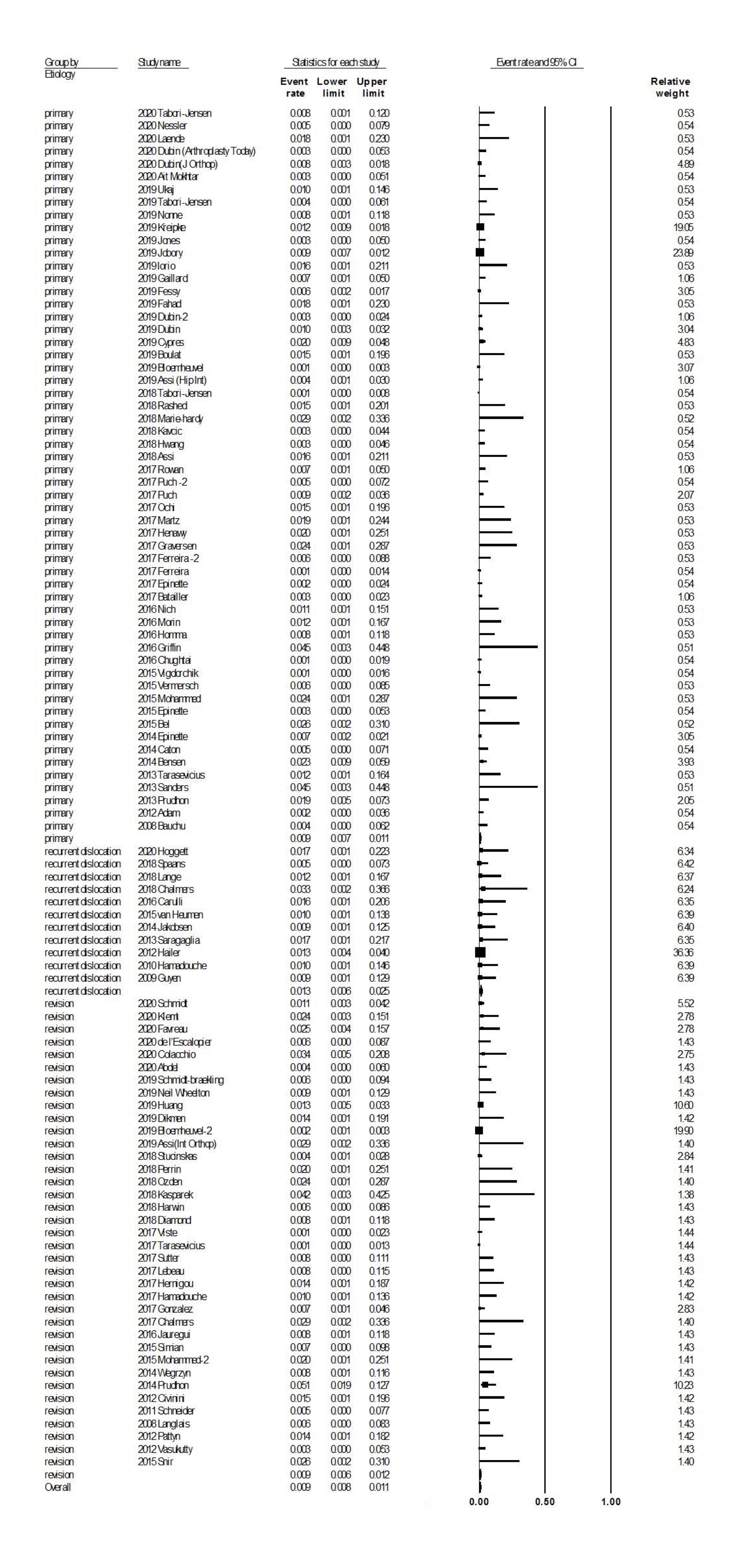
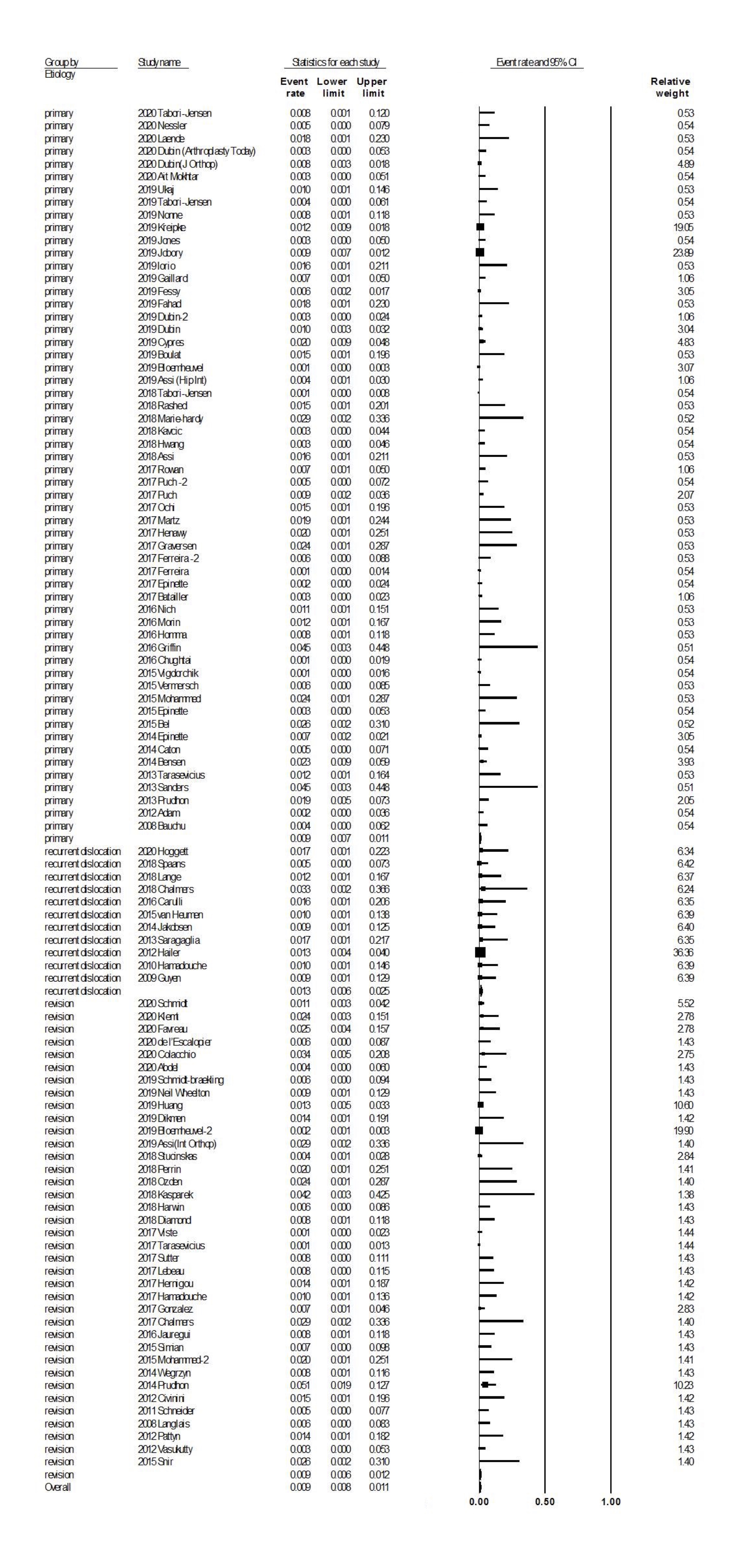
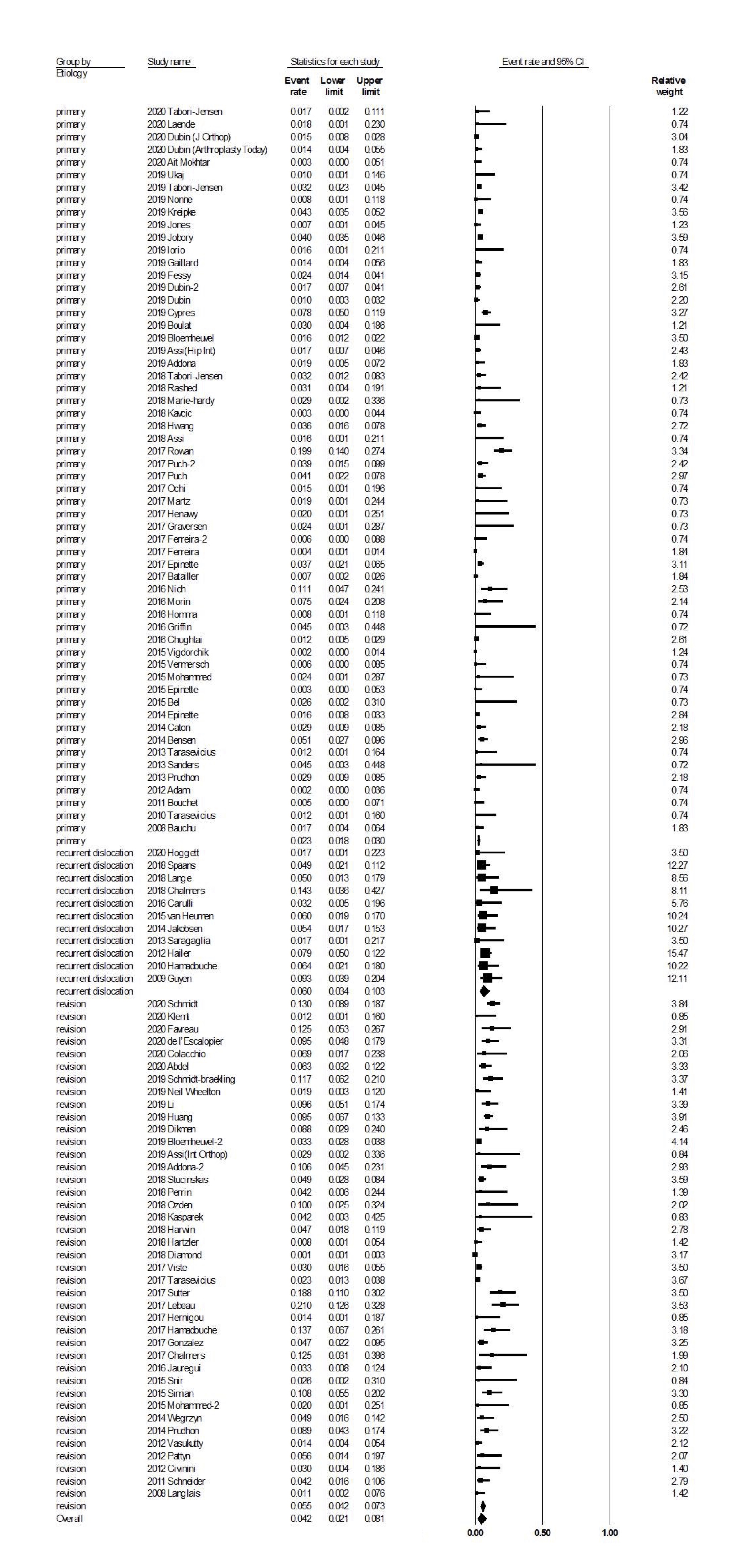
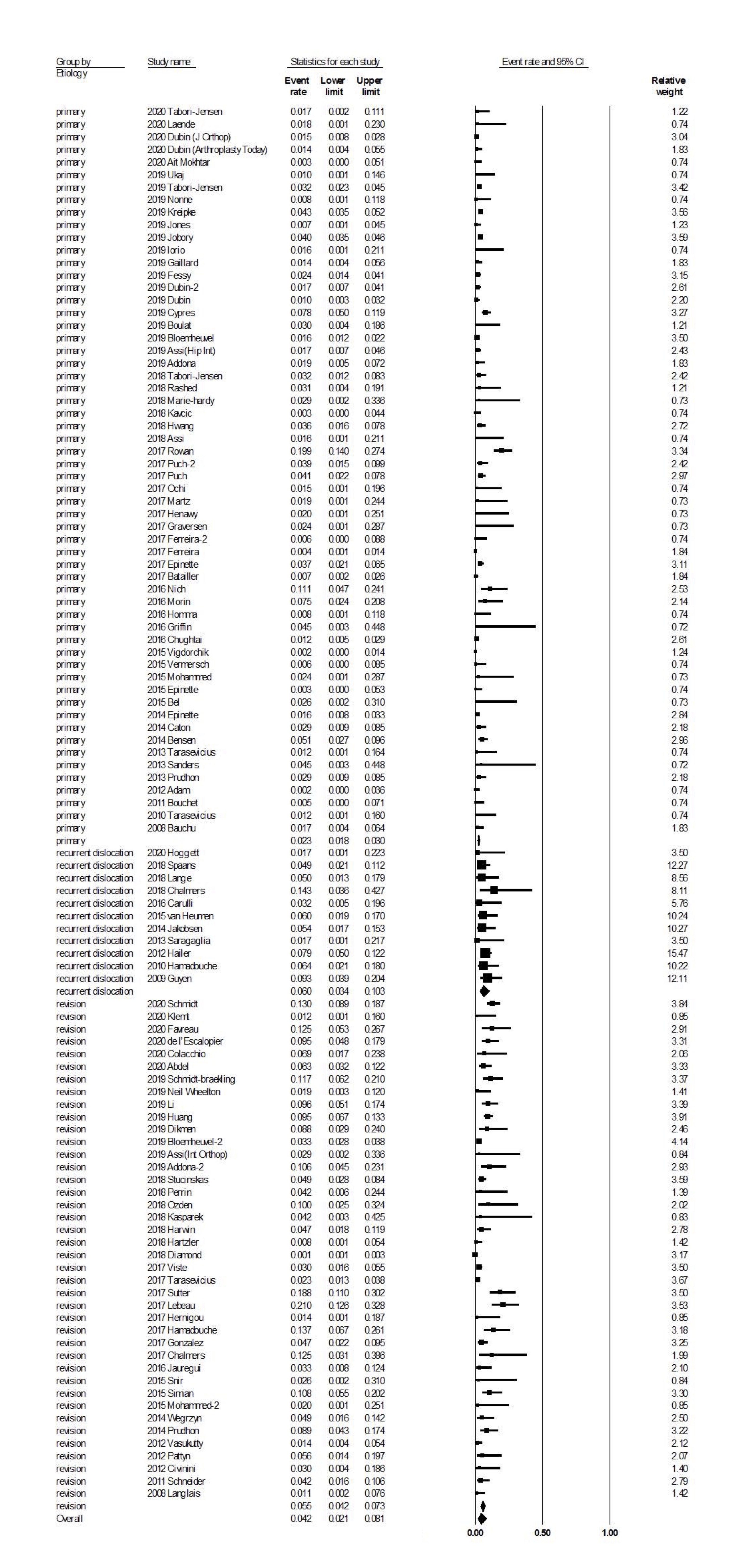
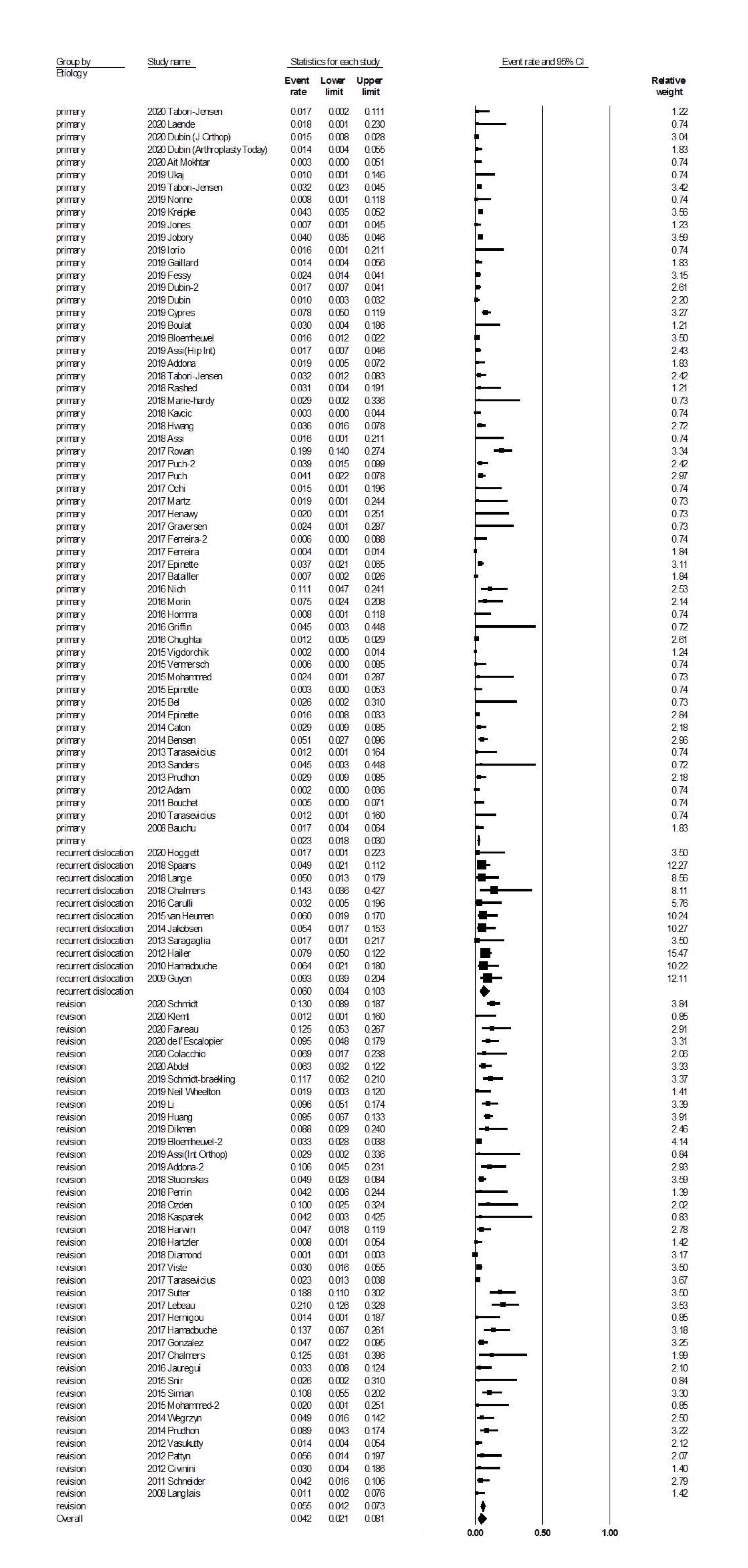
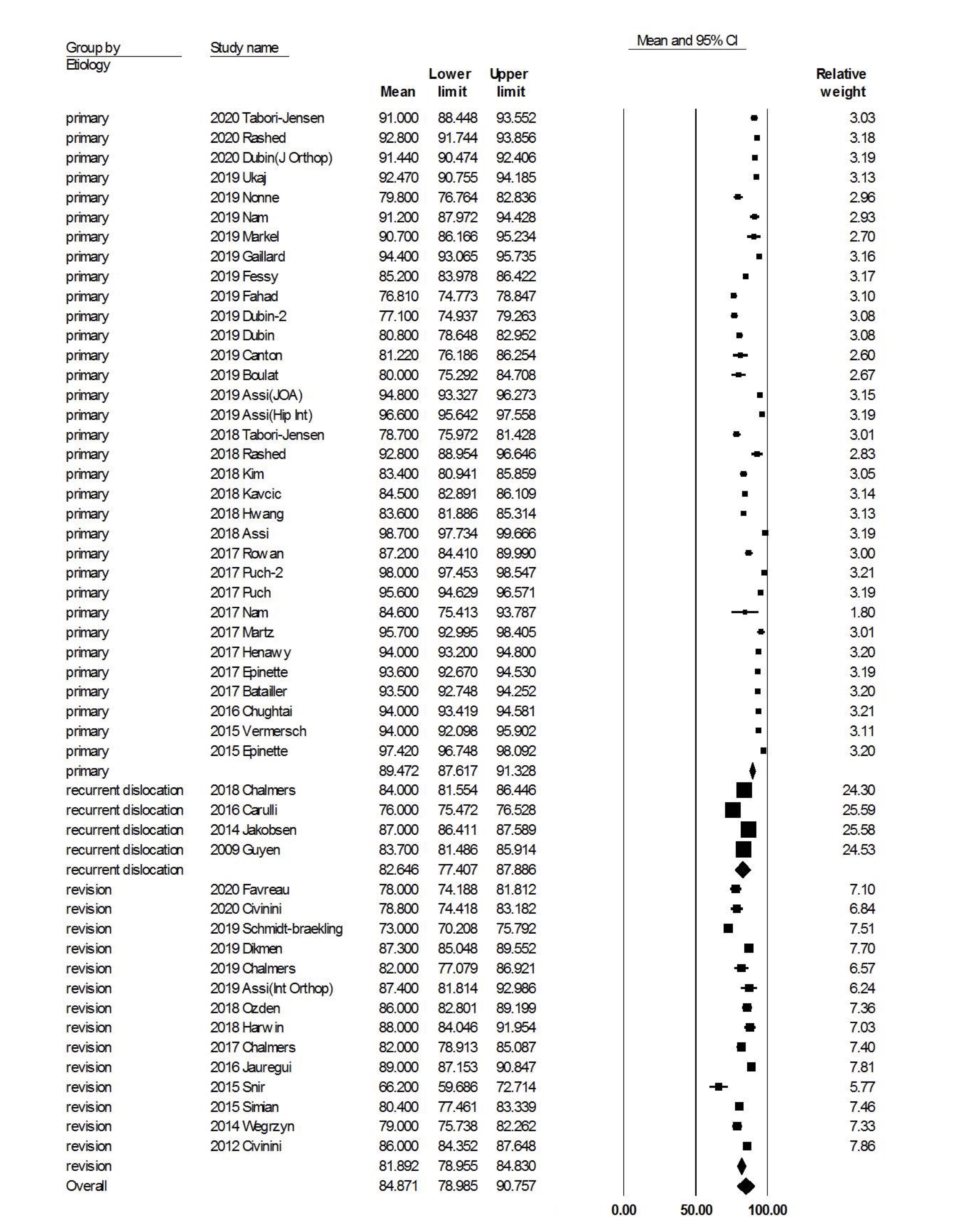
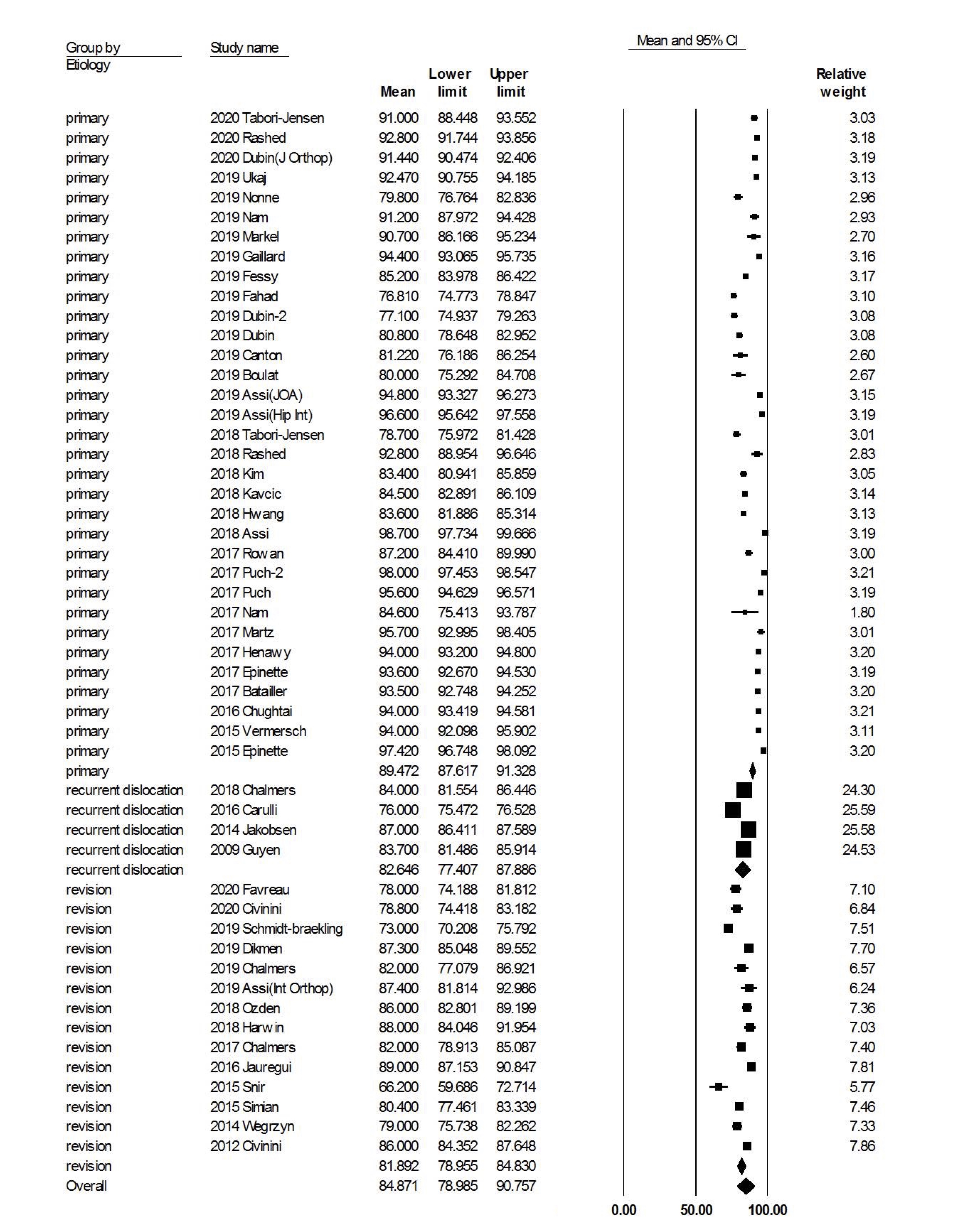
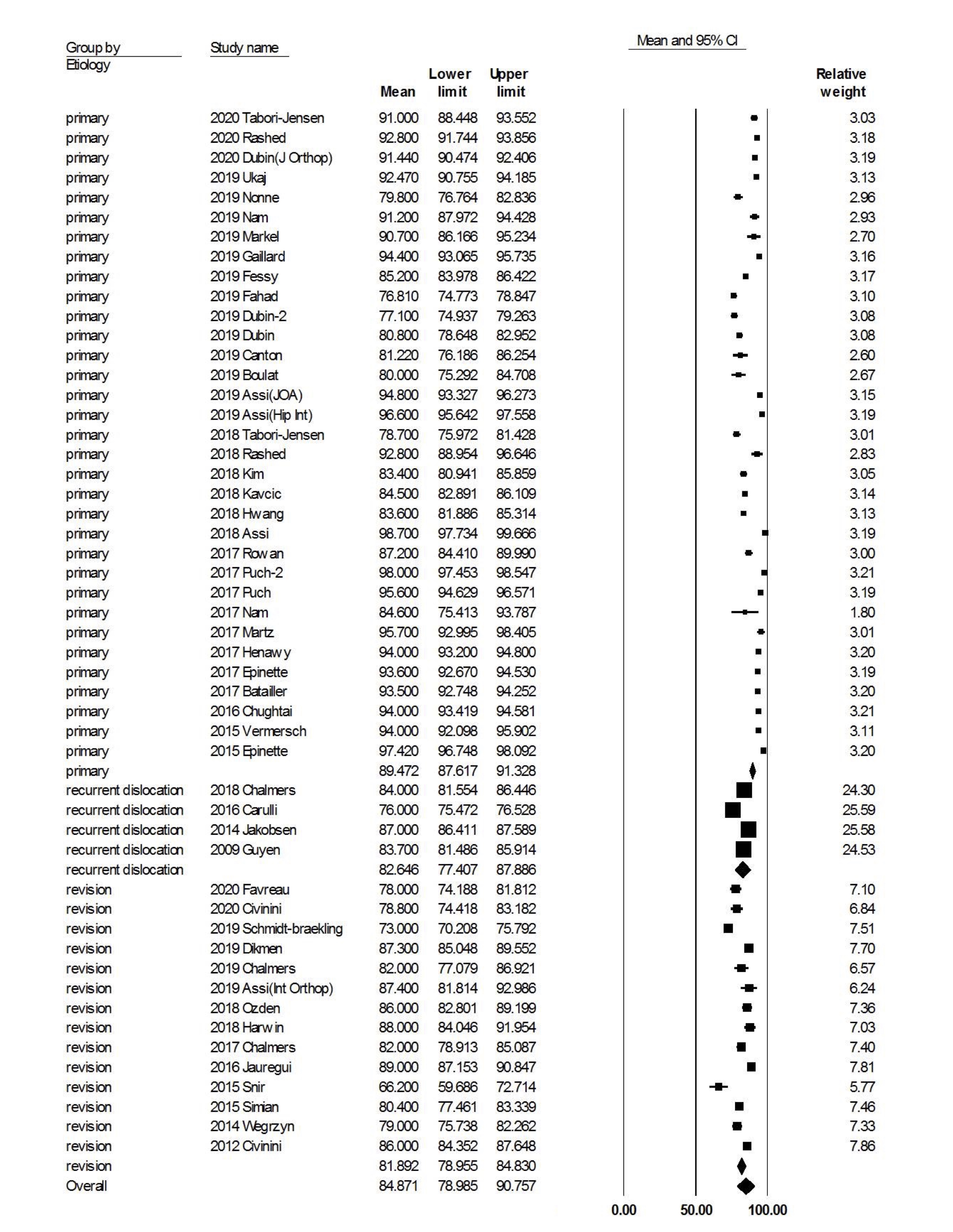
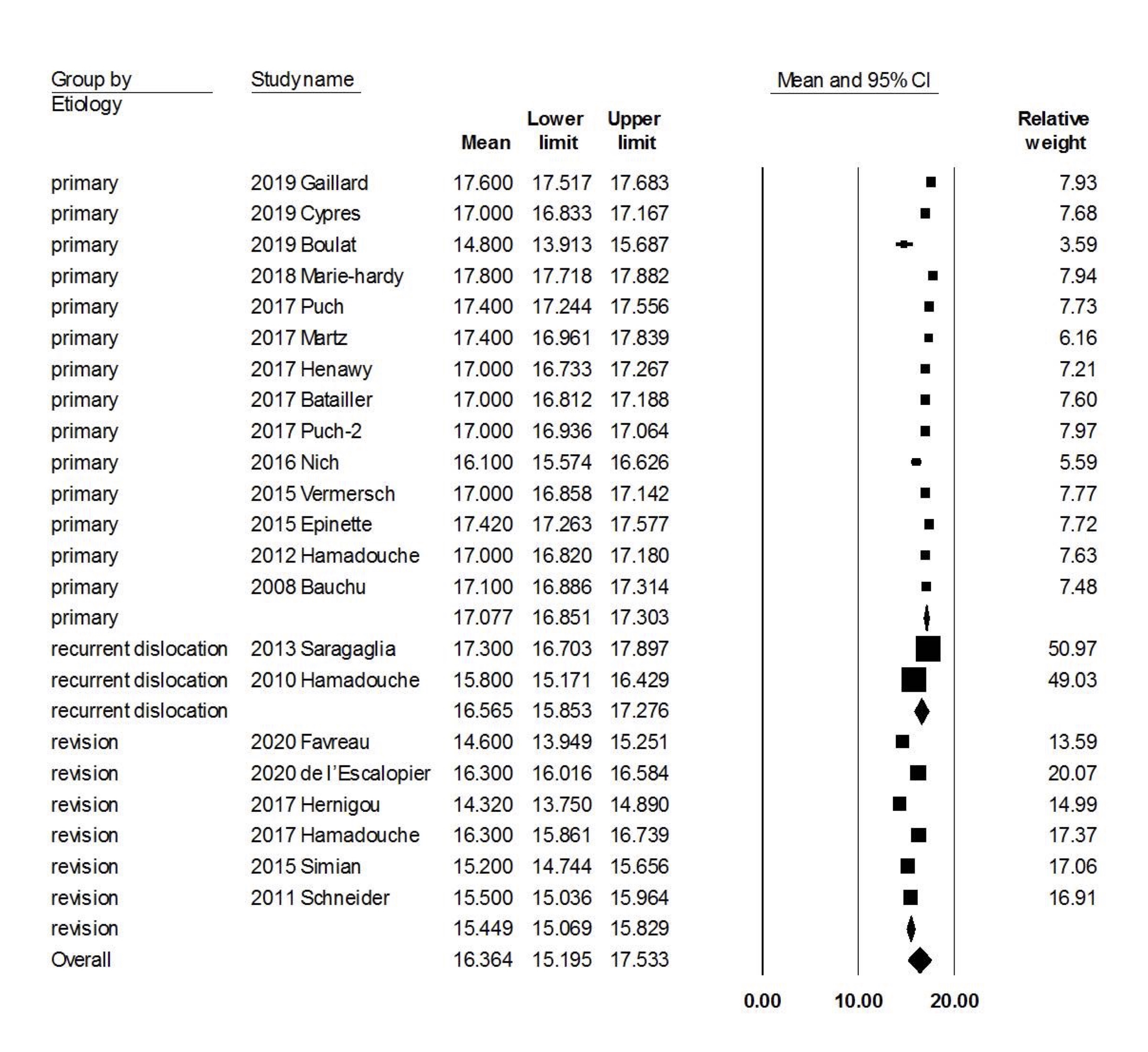
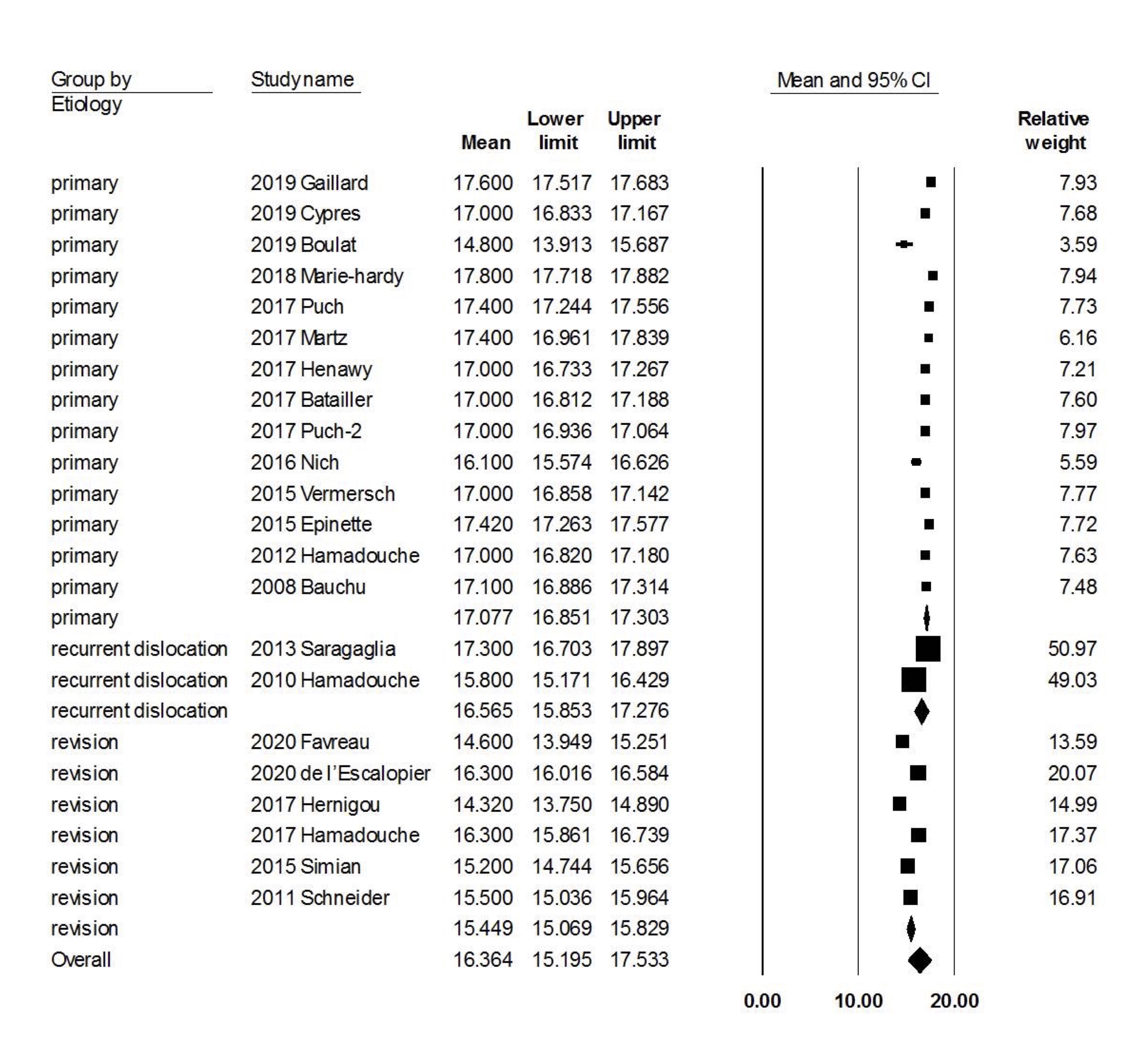
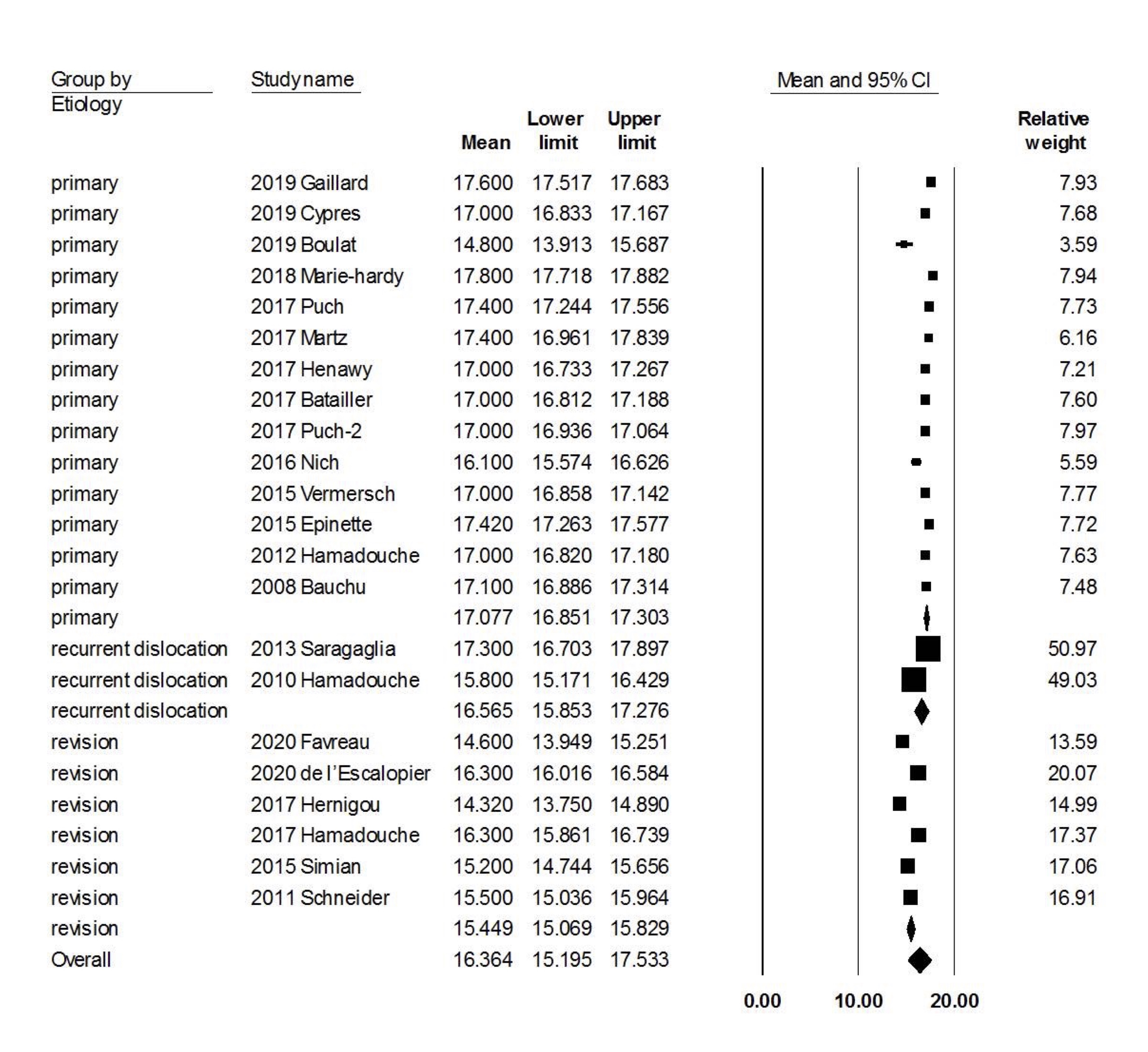
In this meta-analysis, we included 120 studies with 30016 primary and revision THA procedures using the modern DM design. At a mean follow-up of 47.3 months, the overall failure rate of modern dual mobility design was 4.2%. The most common failure modes include aseptic loosening (primary: 0.9%, revision for all causes: 2.2%, revision for recurrent dislocation: 2.4%), septic loosening (primary: 0.8%, revision for all causes: 2.3%, revision for recurrent dislocation: 2.5%), extra-articular dislocation (primary: 0.6%, revision for all causes: 1.3%, revision for recurrent dislocation: 2.5%), intra-prosthetic dislocation (primary: 0.8%, revision for all causes: 1.0%, revision for recurrent dislocation: 1.6%) and periprosthetic fracture (primary: 0.9%, revision for all causes: 0.9%, revision for recurrent dislocation: 1.3%). The multi-regression analysis revealed that revision THA procedures were associated with a higher risk of aseptic loosening, septic loosening, extra-articular dislocation, periprosthetic fracture, overall implant failure and lower Harris Hip scores. But interestingly, several risk factors that have been identified for THA dislocation such as advanced age, female sex, posterolateral approach and increased BMI were not risk factors for extra-articular dislocation. Younger and female patients were associated with higher risk of implant failure. In terms of functional outcome, the patients were satisfied with their postoperative function based on the improved Harris hip score and Merle d’Aubigné score.
Dislocation is one of the common causes of THA implant failure and can be caused by many factors.(8) In current literature, the known risk factors include advanced age, female patients,(9, 10) obesity,(11, 12) previous hip surgeries,(13) posterolateral surgical approach,(14, 15) THA for acute fractures, patients with neurological diseases,(16) and patients with abductor weakness.(17, 18) The dual mobility design increases femoral head-to-neck ratio and jumping distance to improve stability.(20-23) Therefore, we can anticipate decreased dislocation rates for the DM design in primary and revision THA. Even after revision THA due to recurrent instability, the dislocation rate was only 2.5%, which was much lower than the reported dislocation rate after primary THAs and revision THAs, which ranged from 0.3% to 10%(2-4) and 5% to 30%(5-7), respectively. In addition, a multivariate analysis revealed that older age, female patients, posterolateral approach and BMI were not risk factors for dislocation after DM-THA. Based on the difference in risk factors for dislocations, we can assume that the DM design can effectively overcome some of the shortcomings of previous THA designs. Nevertheless, optimization of component position and restoration of soft tissue tension are paramount to prevent dislocation in both primary and revision THA procedures.
Despite these improvements, there are still some concerns with the DM design, including increased wear of the acetabular liner(164), increased risk of aseptic loosening(30) and intra-prosthetic dislocation.(30)
The two-articulation design creates two surfaces for plastic deformation and wear, which theoretically leads to a higher wear rate than fixed-bearing THA. The inner, small articulation dominates the majority of movement and follows the Charnley’s low-friction principle with a small-diameter head to reduce wear.(20) The motion between the outer shell and acetabular component occurs in extreme angle when femoral neck abuts the PE liner and creates a homogenous wear over the liner.(40) Using plain radiographs or implant retrieval analysis, several studies aimed to assess the volumetric difference in wearing of DM articulations and fixed-bearing THA.(165-172) Interestingly, the wear rate of ultra-high molecular weight polyethylene (UHMWPE) bearing in the 1st generation DM cup was less than 40 mm3/year, which was similar to wear rate of UHMWPE in fixed-bearing THAs (30–80 mm3/year at 15 to 21 year follow up).(165-169) In vitro simulation study for modern generation DM cup, using highly cross-linked polyethylene (HXLPE), reported lower wear rate in DM cup compared to fixed-bearing THA (1.2 vs. 2.7 mm3/million cycles, respectively).(170) In another study performed by Laende et al., the wear rate of modern generation DM cups with HXLPE at 3 years follow-up was 0.02 mm/year in DM cup, which was similar to non-dual mobility constructs (0.00 to 0.06 mm/year).(69, 171) In contrast, Deckard et al. recorded the wear rate was two times higher for modern-generation DM cup with HXLPE than the fixed-bearing THA (0.27mm/year and 0.11 mm/year, respectively).(172) The in vitro simulation or retrieval studies have validated reasonable wear rates of DM articulation using either UHMWPE or HXLPE.(165-170) The results from studies using plain radiographs to estimate the wear rate were controversial, which is considered less accurate than the retrieval or simulation studies.(171, 172) Currently, there is limited evidence regarding the increased PE wear of modern DM articulation.
The non-porous alumina-coated surface, tripod anchoring system of acetabular component and polyethylene wear have been associated with a higher aseptic loosening rate in the first-generation DM implants.(24, 29, 31) Several changes have been made in modern dual mobility designs, including (1) to replace UHMWPE with HXLPE to reduce wear(33, 34); (2) to add bevelled edges (or chamfer) in polyethylene (PE) inserts to lower femoral neck impingement and wear(32); (3) press-fit fixation by bilayer coating of porous titanium and hydroxyapatite to enhance osseointegration on the outer surface(31); (4) modular metal liner design to facilitate supplementary screw fixation. The long-term overall survival and aseptic loosening rate of the primary THAs using 1st generation DM implants were 85-95.4% and 3-8.3%, respectively.(24-28) In this study, the primary THAs using modern generations DM implants are associated with a better overall survival (97.7%) and a lower aseptic loosening rate (0.9%). This pooled aseptic loosening rate was comparable to that of primary, fixed-bearing THA from several registries, which ranged from 0.7-1.1% at 5 to 16 years.(1, 173, 174)
The modern, modular design has an additional cobalt-chromium (CoCr) liner inserted into a titanium acetabular component allowing supplementary screw fixation to enhance primary stability. However, the metal-on-metal interface between CoCr liner and titanium cup is at risk of fretting corrosion and remains a concern.(175-177) Metal ions can further lead to advance local tissue reaction (ALRT) and implant loosening.(178) The first study regarding metal ions was conducted by Matsen Ko et al., which revealed 21% of the patient had elevated serum chromium levels.(179) Other studies reported that serum ion levels (cobalt, chromium or titanium) was elevated in 9.3-23% of the patients.(47, 111) On the other hand, some studies have noted that this elevation was not associated with clinical adverse events including instability, loosening or need of revision.(64, 67, 72) In summary, the current evidence suggests there is a slight elevation of serum ion level but this does not negatively affect the implant survival.
Intra-prosthetic dislocation (IPD) is a rare complication of DM design, which occurs as a result of retentive failure of the inner articulation. Long-term, homogenous PE wear or impingement at extreme range of motion between neck and PE liner leads to loss of PE retentive rim and IPD.(180, 181) The incidence of IPD ranged from 0.7%-4.3% in first generation of DM cup and(29, 30) modifications have been made to the 2nd generation DM implants. These changes include a thinner, more polished femoral neck to reduce impingement with the liner and the use of HXLPE to reduce wear during contact.(32) In our pooled study for modern DM cup, IPD rate in primary THA and revision THA was 0.8% and 1.0% respectively, which is much lower than the 1st generation.(29, 30) Another form of IPD has been observed in modern generation DM implants, which often occurs in the short-term. This form of IPD results from a secondary decapsulation of the liner followed by reduction for dislocation.(182) During close reduction of a dislocated DM-THA, impingement occurs between PE liner and posterior edge of the acetabular component. The excessive loading during reduction maneuver may “decapsulate” the femoral head from PE liner. Therefore, the reduction should be performed gradually under general anesthesia with completely relaxed muscle.(29)
Our meta-analysis showed that the mid-term revision rates in primary and revision DM-THA were 2.3% and 5.5-6.0%, respectively. These results were comparable to the reported outcome of primary or revision, fixed-bearing THA.(1, 38, 39, 60, 73, 98, 108, 183, 184) In primary fixed-bearing THA, the mid-term and long-term revision rate ranged from 1.2-4.0% and 12.1-14.3%, respectively.(1, 38, 60, 73, 98, 108, 183) In revision fixed-bearing THA, the mid-term and long-term revision rates can be up to 5.3-13% and 27-45%, respectively.(39, 184)
This meta-analysis revealed promising mid-term outcomes and a reduction in dislocation rate, but the long-term implant survival of modern DM-THA is still lacking. In addition, the regression analysis showed that revision THA procedures, younger age and female patients were associated with a higher risk of implant failure. Younger patients have been established as a risk factor for failure after primary THAs. However, whether female sex is a risk factor remains controversial.(185-188) This can be attributed to the representativeness of the study cohort, follow-up duration and type of implant. Although female patients have been associated with increased risk of dislocation, aseptic loosening, periprosthetic fracture and overall implant failure after primary THA(187, 188), the same was not seen in DM-THA aside from overall implant failure. Potential confounders and inadequate follow-up duration are important considerations when interpreting this result.
We should recognize several limitations. First, we included only studies written in English. In addition, due to the nature of our research question, the level of evidence of the included studies was low (III or IV). Furthermore, we included studies that reported outcome of modern DM (the 2nd and 3rd generation) implants over a time span of 12 years between 2008 to 2020. We could only analyze factors that were clearly described in the studies, including age, sex, surgical approach, BMI and indication for hip arthroplasty. Factors such as surgeons’ experience, patient activity level or implant designs could have affected the outcome but were unavailable could not be analyzed. Nonetheless, this review provides an updated information about the outcome of modern DM implants and factors that might affect the outcome.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}