Study aims and design
Before designing this protocol, we searched the PubMed database for randomized controlled trials (RCTs) of Ⅱb neck dissection in early–stage oral cancer on May 30, 2018, but we found no results. We repeated the search on November 26, 2018, using the keywords “Ⅱb” and “neck” and searching only in English. We found only one RCT with a small sample size, from 2018; and six prospective analyses of Ⅱb after neck dissection, from 2004 to 2018. In addition, we found two retrospective systematic reviews and meta–analyses. All of the above indicated that the rate of Ⅱb metastasis in early–stage oral cancer is extremely low, no more than 6%. However, there is still no strong evidence to prove the necessity of Ⅱb dissection in T1–T2N0M0 OSCC.
We are conducting a parallel–group, non–inferiority randomized trial to assess whether Ⅱb neck dissection should be performed in T1–T2N0 OSCC and its impacts on OS and HRQoL. Our study plan is summarized in Figure 1.
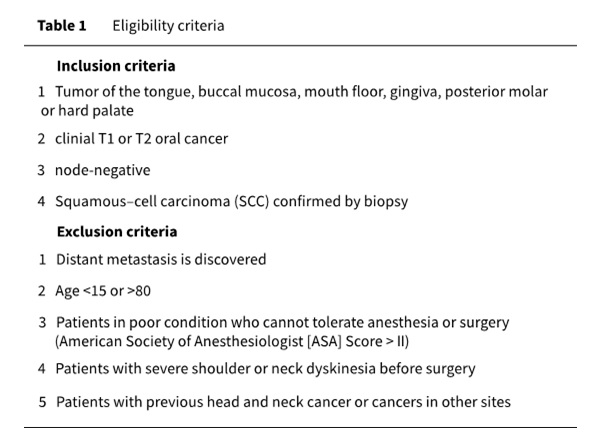
Eligibility criteria
In this prospective, randomized, non–inferiority trial, only patients who are in the clinical stages of T1–2N0M0 according to the American Joint Committee on Cancer (AJCC) Cancer staging Manual, 8th ed.,18 will be enrolled. Based on the NCCN guideline,19 the treatment of T1–T2N0 oral cancer is primary resection with or without ipsilateral or bilateral cervical lymph node dissection or sentinel lymph node biopsy, and radiotherapy or chemotherapy is decided upon according to the specific circumstances. Patients with T2+ stage oral cancer are often recommended postoperative radiotherapy19 and a broader range of neck dissection. Radiation may affect the sensory and motor function of the shoulder, and it has been shown that >90% of breast cancer patients have shoulder pain and motor dysfunction after radiotherapy.20 If clinical T stage >2, the probability of neck occult lymph node metastasis is greatly improved.17 Therefore, we will enroll patients in stage T1 or T2. There may be discrepancies between post–operative pathological T (pT) stage and clinical (cT) stage, as some tumors can be pre–surgically staged as T1 or T2 but stage T3 is confirmed after surgery because of its deep infiltration depth. We have decided to enroll these patients. The treatment principle for tumors located in an oral–cavity site such as the soft palate, tonsil or root of the tongue is different from that for oral cancer.19 Although it is reported that level IIb of the neck can be preserved in T1–T2N0 oropharyngeal cancer,21,22 such patients should not be enrolled. We will eliminate all patients in stage cN+ because the possibility of the occult metastasis in IIb increases.17 Neck status is usually evaluated by bilateral cervical B–ultrasound and enhanced CT/MRI. Patients who have no suspicious lymph nodes will be enrolled after all such examinations have been conducted. In addition, patients with distant metastases should not be enrolled.
Inclusion and exclusion criteria are summarized in Table 1.
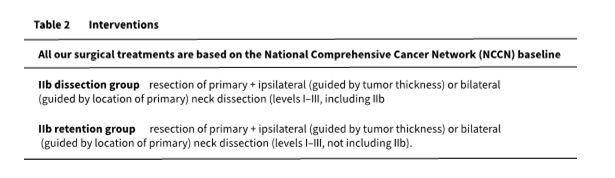
Interventions
After randomization, the two groups will be allocated to different interventions (See Table 2 for details). Primary resection will be 1.5–2 cm away from the tumor, and the negative margin must be attained. During neck dissection, if suspicious nodes in level Ⅲ are found and metastasis is confirmed according to the examination of frozen biopsies, we will expand neck dissection to level Ⅳ or Ⅴ. For the Ⅱb retention group, if a suspicious positive lymph node is found in level Ⅱa during surgery and metastasis is confirmed by frozen examination, both level Ⅱa and Ⅱb must be dissected.5,13
All our surgical treatments will be based on the National Comprehensive Cancer Network (NCCN) baseline.
Outcomes
Primary outcome: overall survival (OS)
We will use the 3–year OS after surgery as the primary outcome, and follow–up at 3months, 6months, 1year, 1.5 years, 2 years, 2.5 years and 3 years after surgery (Figure 2).
Secondary outcomes:
- Health–related quality of life (HRQoL). We will use the Constant–Murley scale to evaluate patients´shoulder function, with follow–up at 7 days, 21 days, 3 months, 6 months, 1 year, 2 years and 3 years after surgery.
- Progression–free survival (PFS). There are many reasons for setting OS as the primary outcome. First, it is widely used as a reliable indicator for evaluating the prognosis of tumors. It is reported that the 3–year OS rate in an Ⅱb dissection group is about 80%,1 which includes disease–free survival and living with disease. Metastasis in level Ⅱb is extremely low, and even if it happens it is nonlethal and can be instantaneously controlled by surgery or radiotherapy. Theoretically, 3–year OS in the Ⅱb retention group will resemble that in the dissection group. A summary of 38 randomized controlled trials (RCTs)7,23 reports no significant association between PFS duration and HRQoL. In addition, as PFS is not as reliable as OS and can also increase difficulties in follow–up, we did not use PFS as the primary outcome.
Participant timeline
- Period −t: recruitment
At the clinic, patients will be preliminary screened. The number of all eligible patients will be represented as n. After eligibility screening, we will record the number of cases that do not meet inclusion criteria as m, and the number of patients to be enrolled will be represented as n1 = n − m. The number of patients who are not willing to sign the informed consent form as m1, and they will be excluded. All patients (n2 = n1− m1) who will accept to participate will be randomized according to a repeatable randomized–number table produced by statisticians.
- Period 0: randomization
This is the starting point of our trial, indicating when patients officially enter it. Patients will be enrolled in the Ⅱb retention or Ⅱb dissection group according to the repeatable randomized number table.
- Period t1: intervention
The number of patients who must be removed from our trial for any reason during intervention (surgery) will be represented as m2, and the number of patients during follow–up will be represented as n3 = n2 − m2.
- Period t2: follow–up
Follow–up timepoints include immediately, 7 days, 1 month, 6 months, 1 year, 1.5 years, 2 years, 2.5 years and 3 years after surgery. Follow–up will include physical examination, enhanced CT/MRI, bilateral neck B–ultrasonography, Constant–Murley score and the safety observation. There will be different evaluations at different timepoints, but overall evaluation will be the same between the two groups. The number of patients who quit our trial for any reason during follow–up will be represented as m3, and the number of patients who will be included in our analysis will be represented as n4 (See Figure 3 for details).
Sample size
In calculating sample size, we assumed the 3–year OS rate in the Ⅱb retention group will be about 78%, α = 0.05 (1–sided), power of 80% (β = 20) and that in the Ⅱb dissection group will be 80%.1 The non-inferiority margin will be 12%, so the sample size as generated by PASS Sample Size Software 15.0 (NCSS LLC, Kaysville, Utah, USA) will be 261 for Ⅱb retention and 260 for Ⅱb dissection. In order to attain a reasonable sample size and make sure the trial is instructive for clinical work, we combined the common opinions of oral and maxillofacial experts, and the statistician defined the non-inferiority margin as 12%.24 Although the value seems to be large, its role is to control the large sample size that would otherwise be unapproachable.
Assignment of interventions
A statistician will write randomized code to generate a repeatable randomized number table. To reduce the predictability during enrollment, the statistician will determine block length, and a team that is not involved in our trial will keep all the blind codes safely. This team will create opaque sealed envelopes according to the randomized–number table, and we will distribute patients according to this table.
Stratification
OS can be affected by many factors, such as T stage (T1, T2) , primary subsite (tongue, buccal mucosa, mouth floor, gingiva, posterior molar region or hard palate) , depth of invasion.25 To balance the number of patients between groups and minimize the bias of the trial, we will use T stage and primary subsite as stratification.
Blinding
Since the intervention in this clinical trial is a surgical procedure and the surgical records can be queried, surgeons and patients know the specific grouping information. After trial we will send data to statisticians and blind to this evaluator.
Data collection methods
Primary outcome
Patients will be followed up by phone on their survival status at each timepoint during period t2, as shown in Figure 2. After 3–year follow–up of the last patient is complete, we will calculate the 3–year OS rate of both groups.
Secondary outcomes
1.Health–related quality of life (HRQoL). We will use the Constant–Murley scale to evaluate shoulder function at each follow–up timepoint. In order to improve the reliability of shoulder function evaluation, two clinicians will be systematically trained on use of the scale.
2. Progression–free survival (PFS). Observation will start at time of randomization and end when events (see below) occurred. In the period of time from stage 0 (Figure 3) to primary recurrence, local metastasis, distant metastasis, and other life–threatening events or death will be defined as PFS.
If a patient has not returned to the clinic for more than two months after the follow–up timepoint, a telephone inquiry will be conducted.
Data management
All paper versions of the original materials will be photographed and saved in an encrypted public database. All electronic data will be stored in the electronic medical records of the Shanghai Ninth People's Hospital. All procedures for evaluating shoulder function will be filmed and saved.
Statistical methods
1.Overall survival
This trial will be terminated when the last patient has been followed up on for 3 years. After the trial ends, the primary end points will be tested by means of two-sided log-rank tests.
2.Health–related quality of life (HRQoL)
We will use a repeated analysis of variance (ANOVA) measure to analyze changes in Constant– Murley score between the 2 groups. It is reported26 that about 67% of patients have shoulder syndrome after neck dissection even if the accessory nerve is spared. Currently, two methods might work to deal with the problem of shoulder dysfunction. The first is to restore the damaged nerve with such methods as intraoperative brief electrical stimulation of the spinal accessory nerve (BEST SPIN). However, this technique has little effect,27 and literature on treatment of damaged accessory nerves is rare. The second is retention of level Ⅱb during surgery in order to preserve the integrity of accessory nerve function and structure. By measuring changes in the action potential of the accessory nerve during surgery, it was found that level Ⅱb dissection can greatly damage the accessory nerve.6 We will use the Constant–Murley scale28 to assess shoulder function. Although the scale’s reliability in evaluating shoulder function has been questioned,29 it has been clinically applied for more than 30 years, and it can reflect both subjective indicators (such as pain or daily activity) and objective standards (such as the muscle mobility and power). Because of the tissue defect caused by primary resection, distant free or adjacent flaps are used to restore it. In order to ensure the flaps alive, movement control after surgery is crucial. Patients with free flaps are clinically permitted to lift the upper body on the 5th day after surgery and can also to sit up in bed. On the 6th day after surgery, mild activities such as walking are permitted. Therefore, the first timepoint for evaluating shoulder function will be the 7th day after surgery, and then there will be follow–up at 1 month, 6 months, 1 year, 2 years and 3 years.
3. Progression–free survival (PFS)
We will use a two-sided log–rank test to check the difference in PFS between the two groups.
4.Others
In addition, we will use post hoc subgroup analyses on the basis of histological factors that were known to have effects on survival, such as death of invasion of the primary tumor.
Harms
Patients will be informed of all surgical risks and adverse effects of intervention before surgery, which will be performed only if the informed consent is signed. The Ethics Committee of Shanghai Ninth People´s Hospital will be notified of any accidents (such as hemorrhagic shock, myocardial infarction, or death) that occur during surgery.
Primary recurrence or neck/distant metastasis (bone, lung) may occur in both two groups. We will expand tumor resection if primary recurrence happens and perform radiotherapy or neck dissection depending on the tumor size. If Ⅱb metastasis is detected during follow–up in the retention group, we will dissect level Ⅱb and perform radiotherapy if necessary. If level Ⅳ or Ⅴ is affected, we will perform additional ipsilateral or bilateral neck dissection, plus radiotherapy or chemotherapy later if needed.
{kind=link}
{kind=link}