Clinical characteristics of patients with primary lesions and paired BMs
The primary lesions of the 11 patients, included in our study (Table 1), were located in lung (7 cases), breast (1 case), kidney (1 case), stomach (1 case) and colon (1 case). All patients received primary tumors and BMs surgeries, and all tumor specimens were available. Therein, Case 3 underwent 4 times BMs surgeries within a time spanning up to 54 months (Figure 1A, B), and two independent brain metastatic specimens were obtained from Case 8. A cohort of 26 tumor specimens was analyzed (number of primary tumors and BMs, 11 vs. 15). The median overall survival time diagnosed with BMs was 22 months (range, 2-62 months). Traditionally, we share a viewpoint that the occurrence of BMs always represents the terminal stage of tumor development. However, recent studies implicated that the dissemination of primary tumors can occur at every stage of tumor progression(Birkbak and McGranahan 2020). This cohort of cases also supported the latter perspective. Part of the cases (4/11) developed disseminated BMs at the very early stage of lung cancer (Table 1). Those 4 patients first manifested as the symptoms of headache. The 4 patients underwent surgery for BMs, followed up receiving primary lesions surgery, with interval times 0.5 to 35 months. The remaining 7 patients all received the primary lesion surgery, and BMs emerged with different intervals when patients manifested as CNS clinical presentation, and the surgery of BMs resection followed. Additionally, there were no more than 3 intracranial metastatic lesions when deciding to perform BMs surgery.
Table 1
The clinical data of primary tumors and paired BMs.
|
Case No.
|
Exp.ID
|
Age (Years)1
|
Gender
|
Location
|
Interval time
(Months)2
|
Treatment of primary lesion
|
Treatment of metastatic lesion
|
Pathology (Type)
|
OS(Months)
|
Adjuvant therapy3
|
End
|
|
Primary
|
Metastatic
|
Primary
|
Metastatic
|
|
1
|
LC_001
|
60
|
M
|
Lung
|
Lt. Cerebellum
|
-35
|
Biopsy
|
Total resection
|
Poorly differentiated SC
|
AC
|
38
|
RT
|
D
|
|
2
|
LC_002
|
58
|
M
|
Lung
|
Rt. Temporal lobe
|
11
|
Resection
|
Total resection
|
Poorly differentiated SC
|
SC
|
72
|
CT
|
D
|
|
3
|
LC_003
|
57
|
M
|
Lung
|
Rt. Occipital lobe
|
-2
|
Resection
|
Total resection
|
ASC
|
AC
|
54
|
NC
|
D
|
|
LC_004
|
58
|
Lt. Occipital lobe
|
8
|
Total resection
|
AC
|
CT
|
|
LC_005
|
60
|
Rt. Cerebellum
|
31
|
Total resection
|
AC
|
CT
|
|
LC_006
|
61
|
Lt. Cerebellum
|
47
|
Total resection
|
AC
|
CT
|
|
4
|
BC_001
|
37
|
F
|
Breast
|
Rt. Cerebellum
|
41
|
Resection
|
Total resection
|
IDC
|
Poorly differentiated carcinoma
|
43
|
RT+CT
|
D
|
|
5
|
LC_007
|
44
|
F
|
Lung
|
Rt. Temporal parietal lobe
|
-15
|
Biopsy
|
Total resection
|
AC
|
Poorly differentiated AC
|
62
|
NC
|
A
|
|
6
|
KC_001
|
51
|
M
|
Kidney
|
Rt. Frontal lobe
|
124
|
Resection
|
Total resection
|
CCRCC
|
Necrosis
|
146
|
RT+CT
|
A
|
|
7
|
LC_008
|
61
|
M
|
Lung
|
Lt. Frontal lobe
|
8
|
Resection
|
Total resection
|
Poorly differentiated AC
|
AC
|
37
|
RT+CT
|
A
|
|
8
|
LC_009
|
38
|
F
|
Lung
|
Subclavian lymph node
|
0
|
Resection
|
Biopsy
|
AC
|
AC
|
19
|
NC
|
D
|
|
LC_010
|
39
|
Lt. Frontal lobe
|
11
|
Total resection
|
AC
|
CT
|
|
LC_011
|
39
|
Lt. Thalamus
|
11
|
Total resection
|
AC
|
CT
|
|
LC_012
|
39
|
Subclavian lymph node
|
14
|
Biopsy
|
AC
|
CT
|
|
9
|
GC_001
|
48
|
M
|
Stomach
|
Lt. Occipital lobe
|
13
|
Biopsy
|
Total resection
|
AC
|
AC
|
23
|
CT
|
D
|
|
10
|
CC_001
|
62
|
M
|
Colon
|
Lt. Frontal lobe
|
5
|
Resection
|
Total resection
|
Moderately differentiated
AC/MUC
|
AC
|
13
|
CT
|
D
|
|
11
|
LC_013
|
58
|
M
|
Lung
|
Lt. Occipital lobe
|
-0.5
|
Resection
|
Total resection
|
Poorly differentiated AC
|
AC
|
13
|
CT+PD1 inhibitor
|
A
|
| 1 The age of onset, regardless of whether the primary lesion diagnosis prior, or earlier diagnosis of metastases. |
| 2 The value is positive, if treatment of the primary lesion prior to metastases, otherwise the value is negative. |
| 3 Preoperative treatment of brain metastases. |
| Abbreviations: OS. Overall survival; ASC. Adenosquamous carcinoma; AC. Adenocarcinoma; SC. Squamous carcinoma; IDC. invasive ductal carcinoma; CCRCC. clear cell renal cell carcinoma; MUC. mucinous carcinomas; RT. Radiotherapy; CT. Chemotherapy; D. Dead; A. Alive. |
Genomic heterogeneity analysis of primary tumor and paired BMs
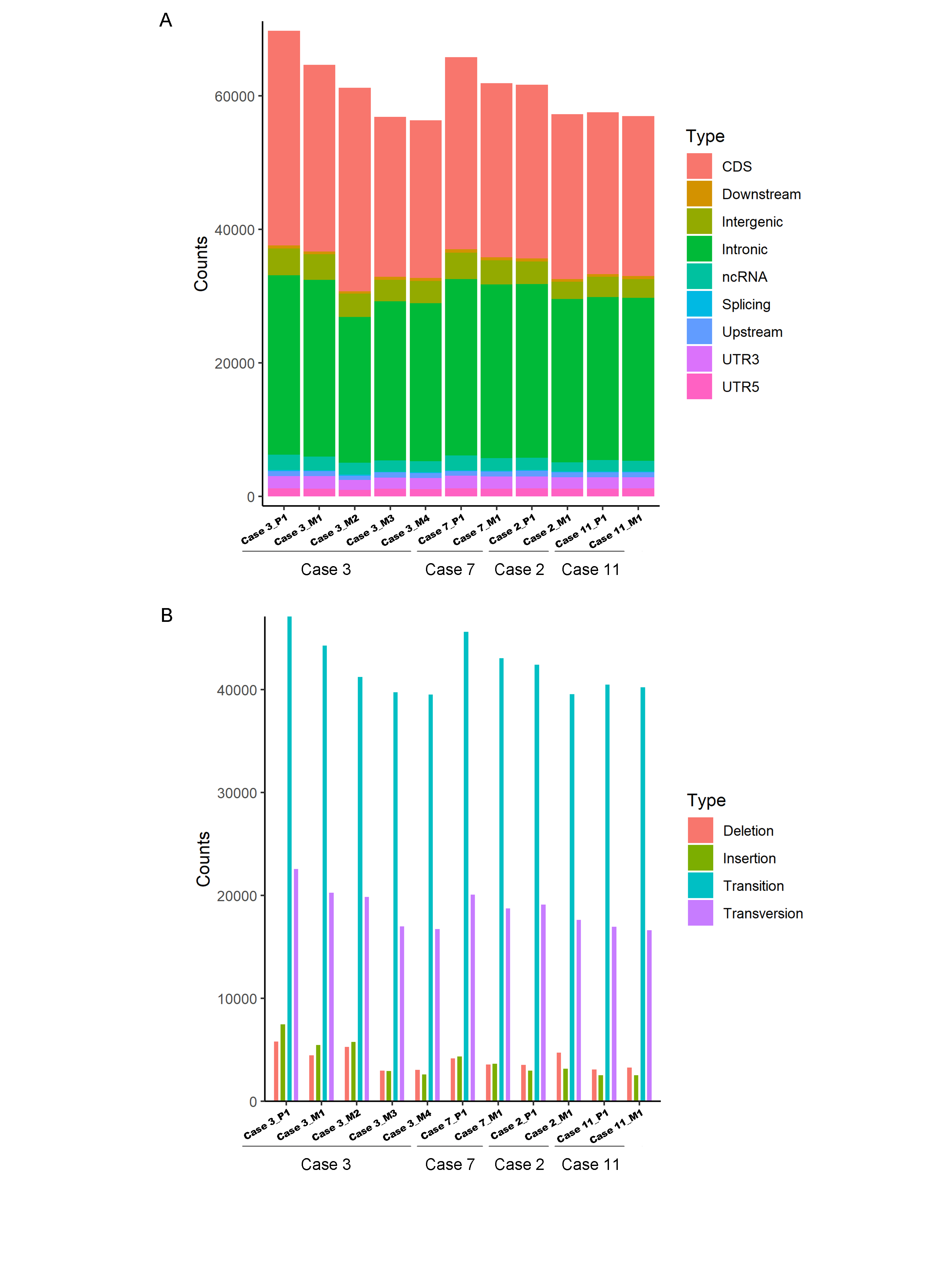
We completed a cohort of 11 paired primary lung tumors and BMs tumor tissues WESeq (Case 2, Case 3, Case 7 and Case 11) (Figure 1B). To assess the genomic variability, the genomic SNPs and InDels of the paired primary and brain metastatic lesions were compared. Consistent with the previous report(Burrell et al. 2013), primary tumors accumulated more genomic variation than BMs (Supplementary Figure 1A, B). Subsequently, we screened the mutation sites for deleterious and compared the primary lesion with 4 brain metastatic lesions in Case 3. We found that SNPs (including missense, stopgain and stoploss) and InDels (including framesShift, stopgain and stoploss) shared a remarkable diversity between the primary lesion and the four divided BMs (Figure 2A). The primary tumor accumulated more deleterious genomic variations (SNP and InDel) than the 4 spatial and temporal divided BMs in Case 3 (Figure 2B), and the shared SNPs and InDels between primary lung cancer and BMs gradually decreased with gone by (Figure 1B and Figure 3A). We also found that compared with the primary tumor, only a small part of SNPs and InDels (ranging from 5.85% in Case 3_M4 to 38.78% in Case 11) (Figure 2C) were shared in BMs. Figure 3B summarized the frequency spectrum of common driver gene mutations. MUC16, PRX and SDHA showed the highest frequency of deleterious mutations, occurring in all primary lung cancers and BMs. It has been reported that the classic tumor marker CA125 encoded by the MUC16 gene played a vital role in regulating tumor cell metastasis(lei et al. 2020), and succinate dehydrogenase (SDH) complex subunits mutations were reported highly associated with tumor cells metastases in pheochromocytoma and paraganglioma and other malignancies(Gill 2018; Lee et al. 2020a).
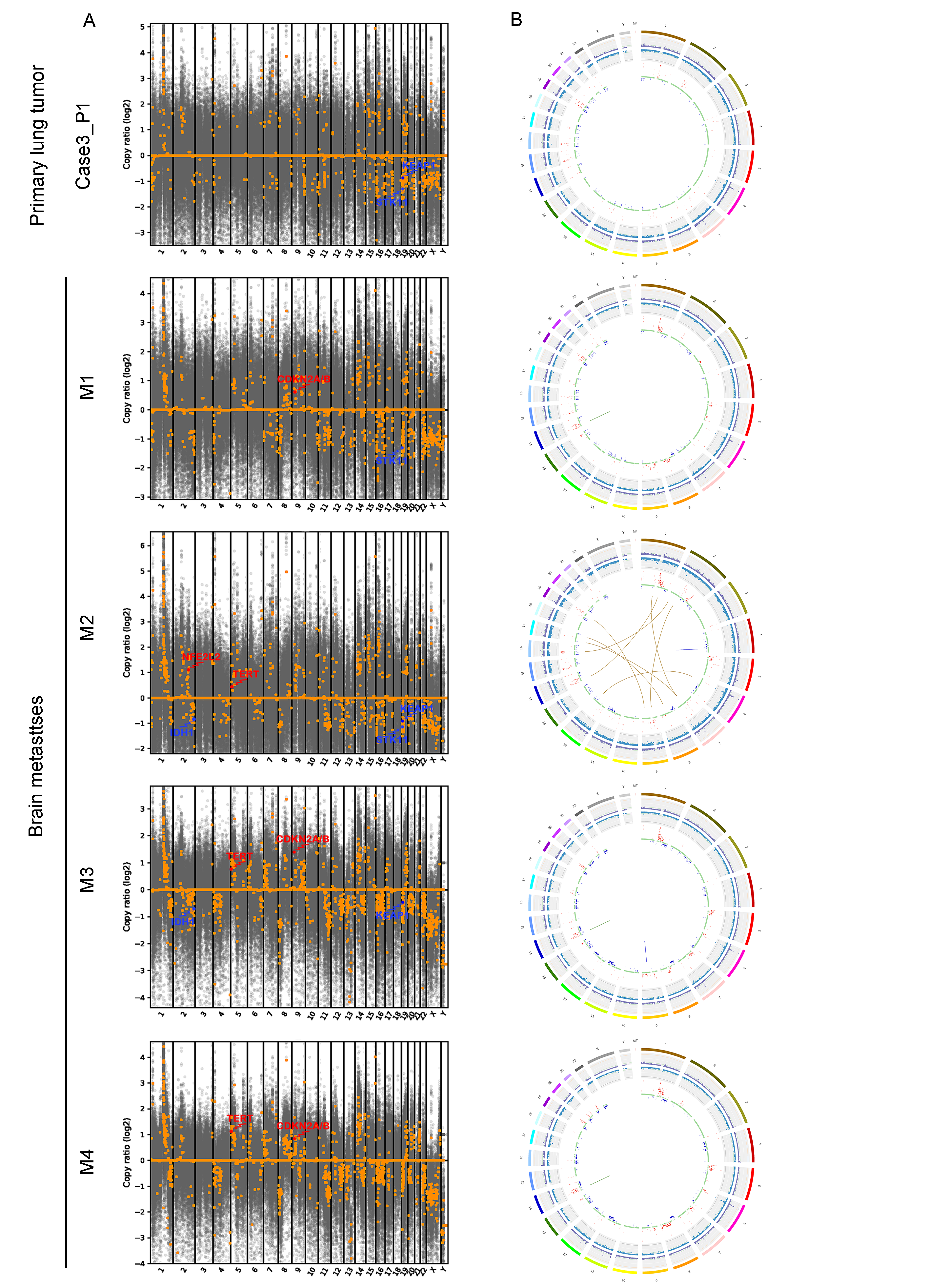
Additionally, CDKN2A/B genes, a set of recognized lung cancer suppressor genes, copy number amplification were observed in M1, M3 and M4 BMs of Case 3, while no aberrations were found in the primary tumor and M2 (Figure 3C). It has been reported that STK11 and KEAP1 mutations were associated with poor prognosis in patients diagnosed with lung adenocarcinoma(Papillon-Cavanagh et al. 2020). Our study also indicated that STK11 and KEAP1 copy number deletions occurred in Case 3 and Case 7, but not all BMs in Case 3 were consistent (Figure 3C). Moreover, CNV events of a cohort of genes, including KRAS, CDKN2A/B and IDH1, were frequently found in brain metastatic lesions (Figure 3C). Supplementary Figure 2 summarized the total genomic fragments copy number aberrations, and common lung cancer- and brain tumor-related genes CNVs were marked. Integrated analysis of the genomic variation of the patient’s primary tumors and BMs, we found that the genomic heterogeneity between the primary tumors and BMs was striking higher than we expected (Figure 3 and Supplementary Figure 2). The Circos diagram revealed that Case 3_M2 showed a significantly higher frequency of chromosomal aberrations (Supplementary Figure 2B), such as interchromosomal translocations. The analysis of cancer cells’ clonal composition in BMs revealed a similar clonal clusters composition in Case 3, with the characteristics of polyclonal dissemination (Figure 4A, B).
Internal histopathologic heterogeneity and evolution analysis
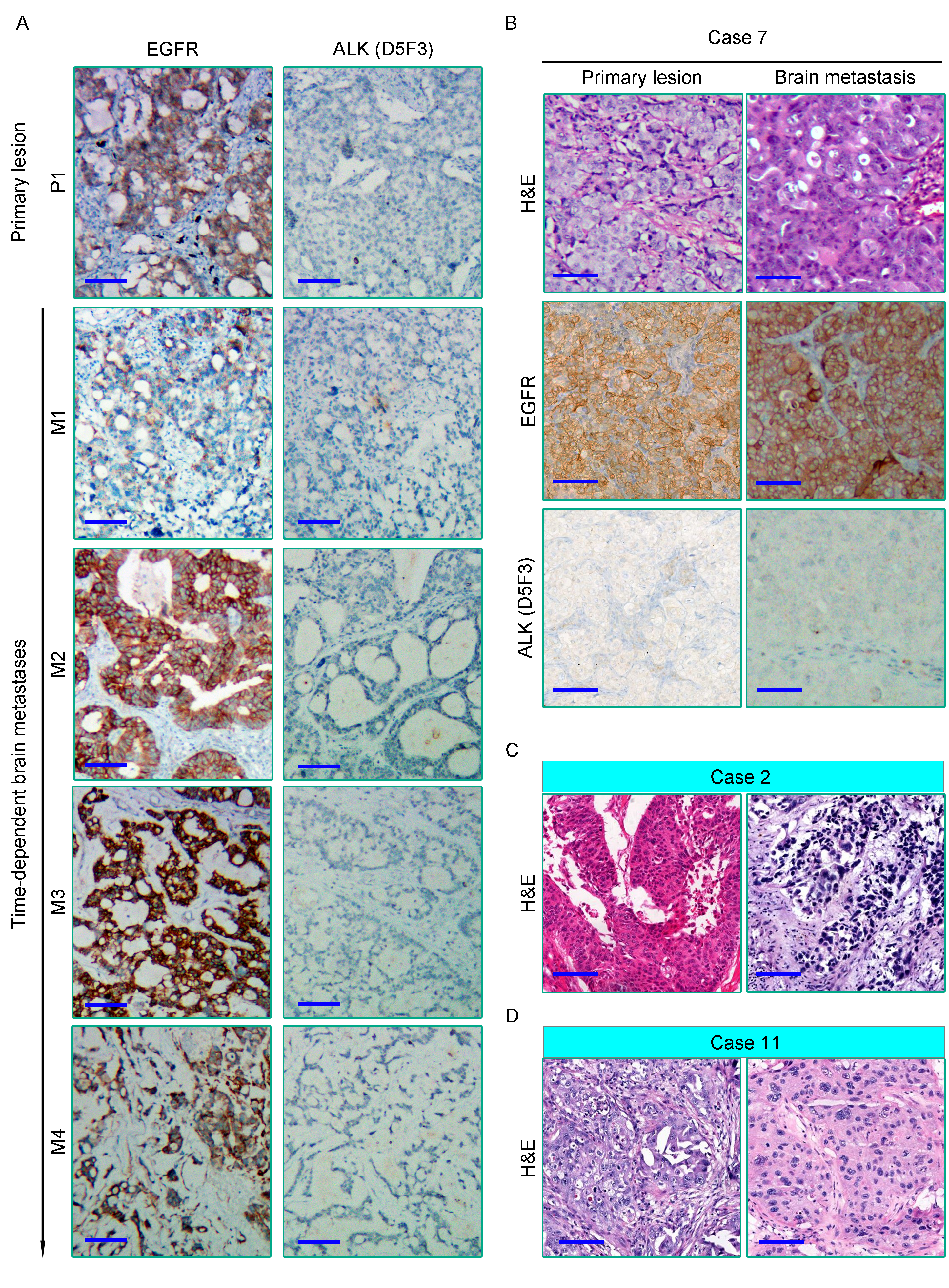
In most cases, the histomorphological differences between the primary lung tumors and BMs were limited (Figure 5A and Supplementary Figure 3B-D). However, we still observed some alterations in Case 3 with multiple recurrences. From foci M1 to M4, it showed a variable level of cancer cell differentiation, from well-differentiated to poorly differentiated. Metastatic lesions still basically maintained the histopathological characteristics of the primary lung cancer at an early stage of dissemination. However, we found a remarkably poorer degree of tumor differentiation in the extremely long-term brain metastatic foci than the primary lesion, with the classic tube-like structure gradually disappeared. Tumor cell clusters were diffusely distributed, and the nucleus atypia, mitosis and giant polymorphic nucleus could be observed frequently in metastatic foci M4 (Figure 5A).
Tumor-related immune heterogeneity between primary lesions and paired BMs
Emerging evidence suggests that brain is not an “immune privileged” organ as previously thought. The immune checkpoint therapy targeting the PD1/PD-L1 pathway has notably improved the survival outcomes of several types of malignant tumors, which also brought hope to patients with BMs. Higher PD-L1 expression of tumor cells and/or TILs density is always associated with favorable anti-PD1/PD-L1 immunotherapeutic efficacy(Ribas and Hu-Lieskovan 2016). However, in contrast with the primary lesions, the efficacy of immune checkpoint therapy targeting PD1/PD-L1 in BMs is indeed not so significant(Goldberg et al. 2016; Kluger et al. 2019). Herein, we assessed PD-L1 expression in a cohort of primary tumors and paired BMs by immunohistochemistry. Our study indicated that the expression level of PD-L1 in metastatic tumor cells was significantly lower than that of paired primary lung cancers (P = 0.0013) (Figure 5).
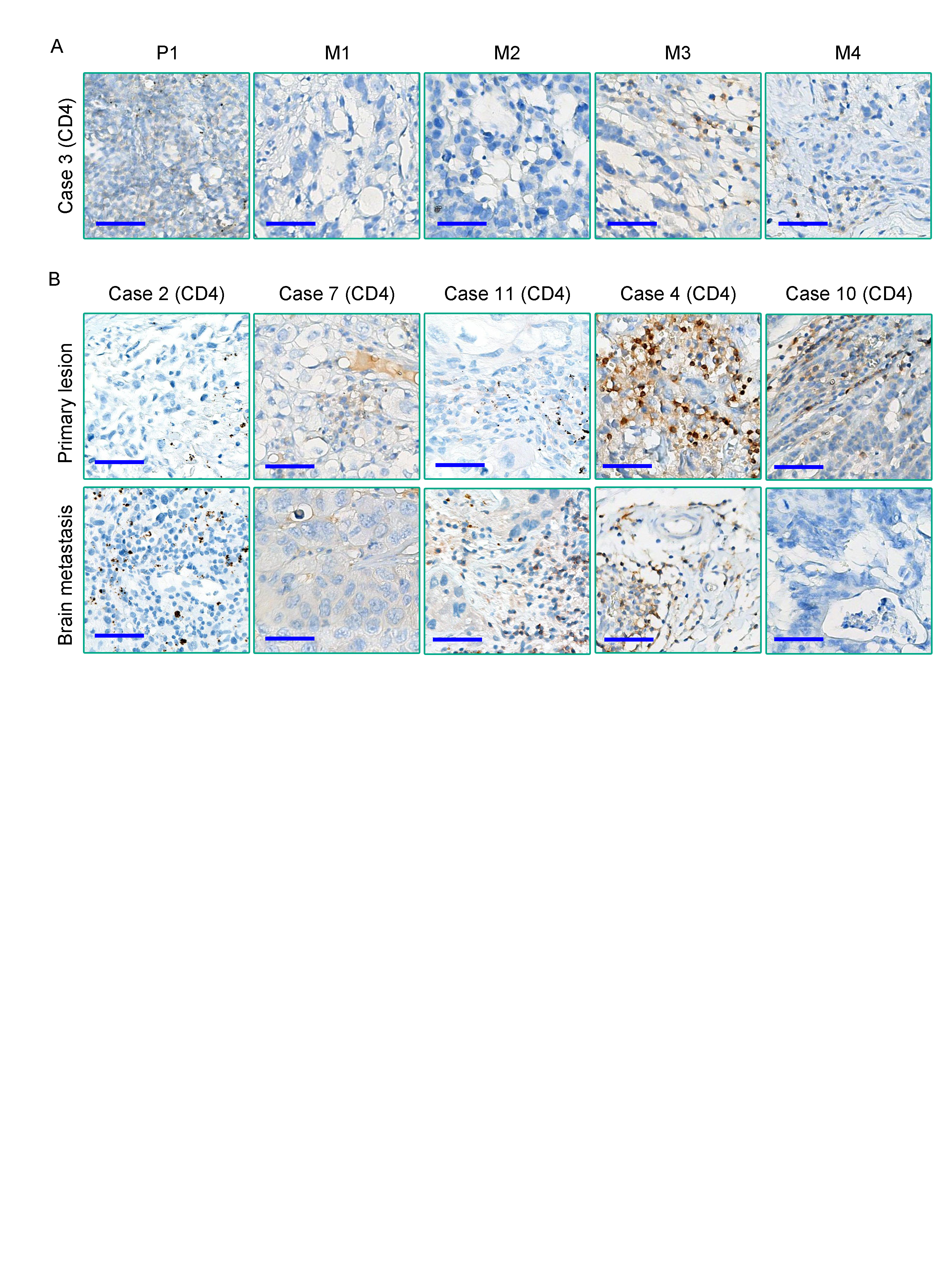
TILs, especially CD8+ TILs, represent a favorable prognostic factor in several types of cancers(Gueguen et al. 2021). Meanwhile, CD8+ TILs performed as the final executor of PD1/PD-L1 pathway. A comparative study on primary tumors and paired metastases revealed that the density of CD8+ TILs in BMs was significantly lower than that of matched primary tumors (P = 0.0248) (Figure 6A-C). Our results also demonstrated a relatively lower density of CD4+ T cells in primary lung cancers (Case 2, 3, 7 and 11) and paired BMs, while the density of CD4+ T cells was higher in breast cancer (Case 4) and colorectal cancer (Case 10) (Supplementary Figure 4A, B). Although only Case 11 was treated with PD1/PD-L1 blockade immunotherapies in this cohort of retrospective study, the above analysis still benefits us to comprehensively insight the immune microenvironment of BMs, provides us novel clues to evaluate the efficacy of immunotherapy of BMs. In summary, BMs differed from paired primary tumors by showing notable immunosuppressive characteristics than primary tumors.
Analysis of immunohistochemical phenotypic heterogeneity between primary lesions and paired BMs
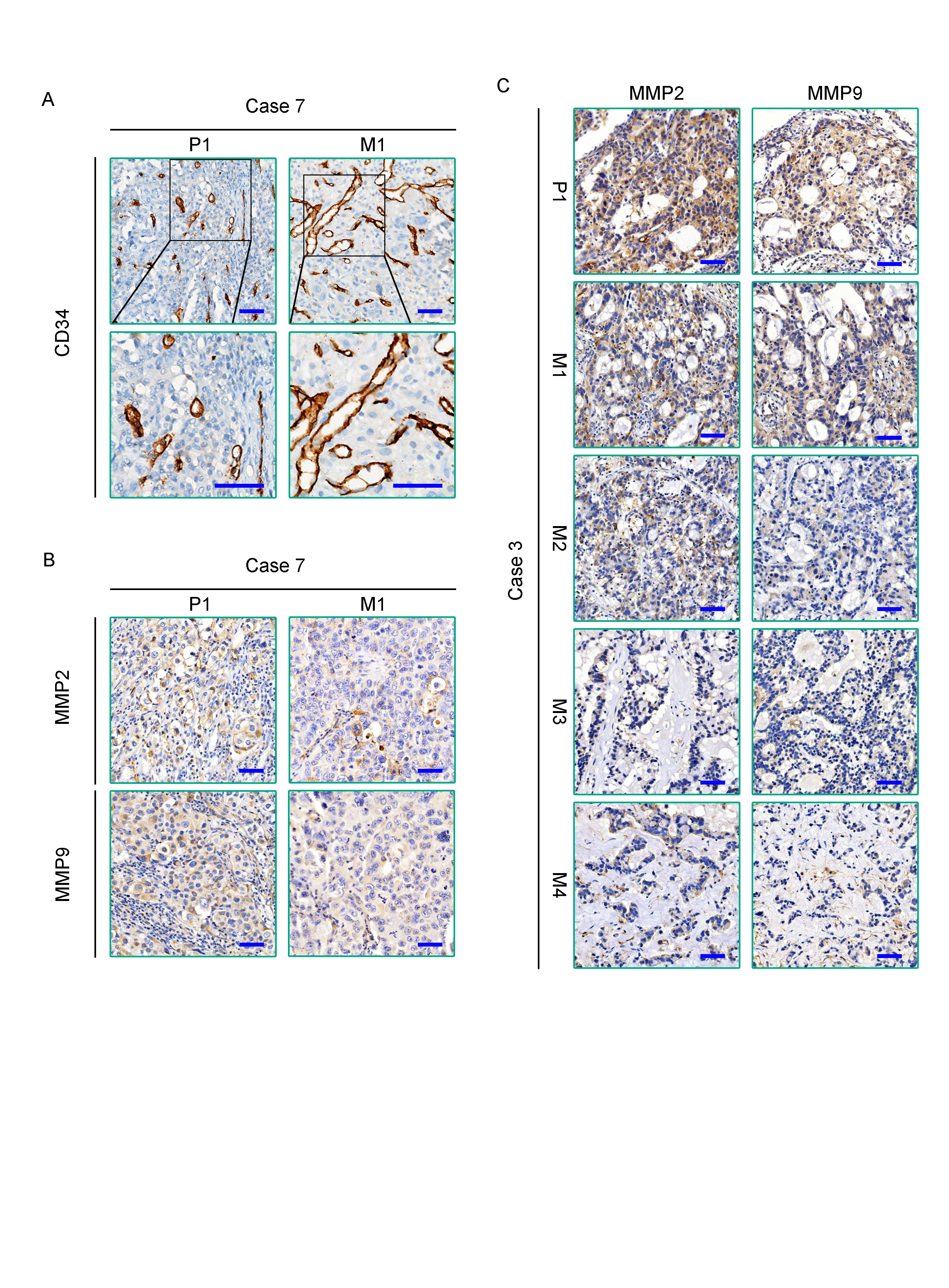
Finally, we integrative analyzed the molecular phenotypes of all 11 primary tumors and paired BMs. Although primary tumors and paired BMs shared pivotal molecular phenotypes, such as the EGFR expression and EML4-ALK fusion status in lung cancer cases (Case 2, Case 3, Case 7 and Case 11), ER, PR, and HER2 expression status in Case 4 (Supplementary Figure 3 and Supplementary Table 1). While comparatively analyzed tumor invasiveness (MMP2 and MMP9 staining) and tumor microvascular density (MVD) (CD34 staining), a notable difference of MVD was found between the primary tumors and paired BMs, and inter-BMs, with tumor MVD more plentiful in BMs than in the paired primary tumors (Figure 7A-C and Supplementary Figure 5A). Meanwhile, the expression of MMP2 and MMP9 in primary tumors was significantly higher than that in metastatic tumors (Supplementary Figure 5B, C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}