The study was approved by The University of Pittsburgh Institutional Review Board. All methods were performed in accordance with the ethical principles stated in the Belmont Report, a requirement of The University of Pittsburgh Institutional review Board. Written informed consent, approved by the University of Pittsburgh Institutional Review Board, was obtained prior to participation. Subjects diagnosed with glaucoma underwent an established assessment of their balance, focused on their abilities to centrally integrate sensory information relevant for postural control.
Participants
Eleven individuals diagnosed with glaucoma were recruited for this study (Table 1). All recruited participants were clinically diagnosed with glaucoma after undergoing a comprehensive ophthalmic evaluation at the UPMC Eye Center that included a clinical exam, visual field testing (Humphrey Field Analyzer; Zeiss, Dublin, CA) and a spectral-domain optical coherence tomography (Cirrus HD-OCT, Zeiss, Dublin, CA). Participants were able to stand for at least 2 hours. Exclusionary criteria were self-reported orthopedic, neurological, pulmonary or cardiovascular conditions that may negatively impact balance and ocular pathologies other than glaucoma. Potential participants were also excluded if they were taking any central nervous system anti-depressant drugs, including benzodiazepines or barbiturates, or taking more than five prescription drugs, as both may increase fall risk [12, 13]. Glaucoma severity was determined two ways: (1) using a functional measure, specifically visual field mean deviation (VF MD) assessed by automated Humphrey perimetry and (2) using a structural measure, specifically retinal nerve fiber layer (RNFL) thickness as measured by OCT.
Protocol
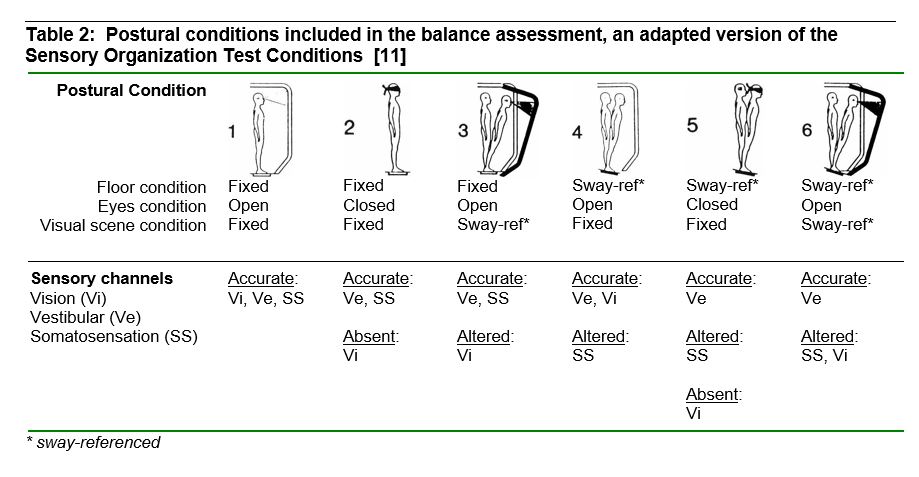
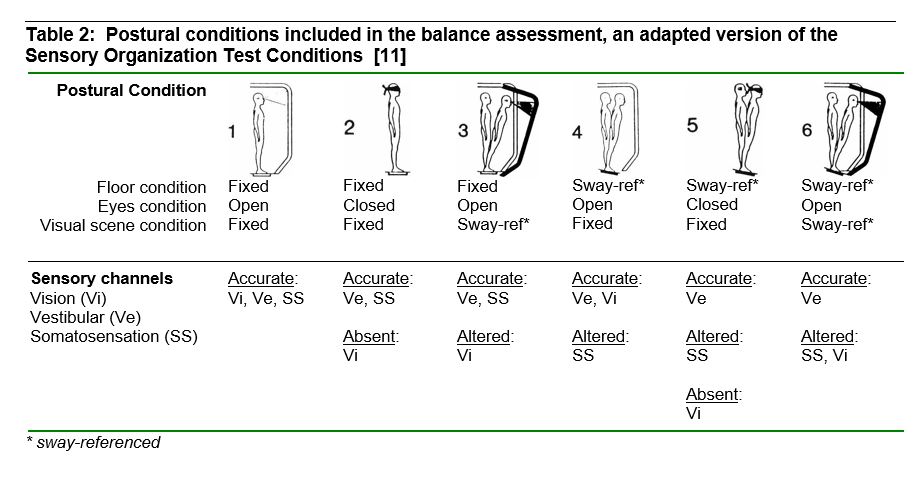
The standing balance test used dynamic posturography on an Equitest posture platform (Neurocom, Inc) located in the Jordan Balance Disorders Laboratory within the Eye & Ear Institute of Pittsburgh. The Equitest platform is capable of sway-referencing the floor and/or visual environmental, which provides rotations of the supporting floor and/or visual scene in direct proportion to an individual’s sway magnitude in the anterior-posterior direction. Sway-referencing the floor causes movements of the supporting surface in an attempt to keep the ankle angle constant, thus reducing and altering somatosensory information from the ankle and requiring the person to rely on vision and vestibular inputs for balance [14]. Similarly, sway-referencing the visual scene in proportion of the individual’s sway will reduce balance-related visual cues. The platform records ground reaction forces under the feet during standing and underfoot center of pressure (COP) is computed and saved during the trials. Participants wore a safety harness that would prevent hitting the floor in the event of a balance loss. During balance testing, participants were instructed to stand as still as possible without locking their knees. Participants were assessed in 6 postural conditions (Table 2), each lasting 3 minutes (an adapted version of the Sensory Organization Test, a well-established balance testing paradigm used and validated in healthy and clinical populations [11]). These sensory challenging conditions alter and/or reduce sensory information relevant for balance in a systematic manner (Table 2).
Data Processing and Analyses
The COP data were low-pass filtered using a fourth-order Butterworth filter with a cutoff frequency of 2.5 Hz, and down-sampled to 20 Hz. The first 30 and last 5 seconds of the COP time series were removed to eliminate any transient effects. Anterior-posterior COP data were used to quantify postural sway since sway-referencing was in the anteroposterior direction. Sway magnitude was assessed using the root-mean-square of the filtered COP displacement (COP RMS). The speed of movement was assessed by using the time-normalized path length of the COP data (COP NPL), calculated by summing the absolute value of the differences over time.
Preliminary analyses were focused on investigating the impact of postural condition (PC1, …, PC6) on sway measures (COP RMS and COP NPL) using a mixed linear model with postural condition as the fixed effect and subject as the random effect. To examine the association between glaucoma severity and balance in the main analyses, mixed linear models were used in JMP Version 10 (SAS Institute Inc), with the fixed effects including a glaucoma severity measure (one of four possible measure as explained below), postural condition (PC1, …, PC6) and the interaction of these factors. Subject was also added as a random effect. Four measures of glaucoma severity were individually considered as independent measures in these statistical models: (1) functional measure of glaucoma severity (VF MD) of the better and worse eye, and (2) structural measure of glaucoma severity (RNFL thickness) of the better and worse eye. The dependent variables of interest in both the preliminary and main analyses were the log-transformation of the sway measures, specifically COP RMS and COP NPL. Both of these measures were log-transformed to satisfy the required normality assumption. Statistical significance was set at 0.05.
{kind=link}
{kind=link}