Study population
This retrospective study included consecutive patients who were diagnosed to have PDAC by pathological examination after pancreatic resectional surgery between 1st December 2017 to 30th December 2018. The inclusion criteria were: (1) PD or DP with curative intention, and (2) underwent a standardize pathological protocol for the resected specimen and a standard reporting record for resection margin (R) status according to the NCCN guidelines for pancreatic cancer. The exclusion criteria were: (1) total pancreatectomy (TP); (2) macroscopic evidence of margin involvement (R2); (3) patients received neoadjuvant chemotherapy; (4) resection for metastatic disease. The Changhai Hospital Review Board approved the study, and no additional informed consent was required to review the patients’ medical records.
Pathological Examination
The Leeds Pathology Protocol (LEEPP) was routinely used [14, 15] for the pathological examination.
For PD specimens:
Briefly, after multicolor inking of the posterior, medial margin, and anterior surfaces of the pancreatic head, the specimen of PD was serially sliced in an axial plane, perpendicular or paralleled to the longitudinal duodenal axis.
For DP specimens:
After multicolor inking of the posterior and anterior surfaces of the pancreatic body and tail, the specimen of DP was serially sliced in a plane parallel to the main pancreatic duct or the pancreatic transection margin when the tumor invades to the surface of the pancreas according to the NCCN guidelines.
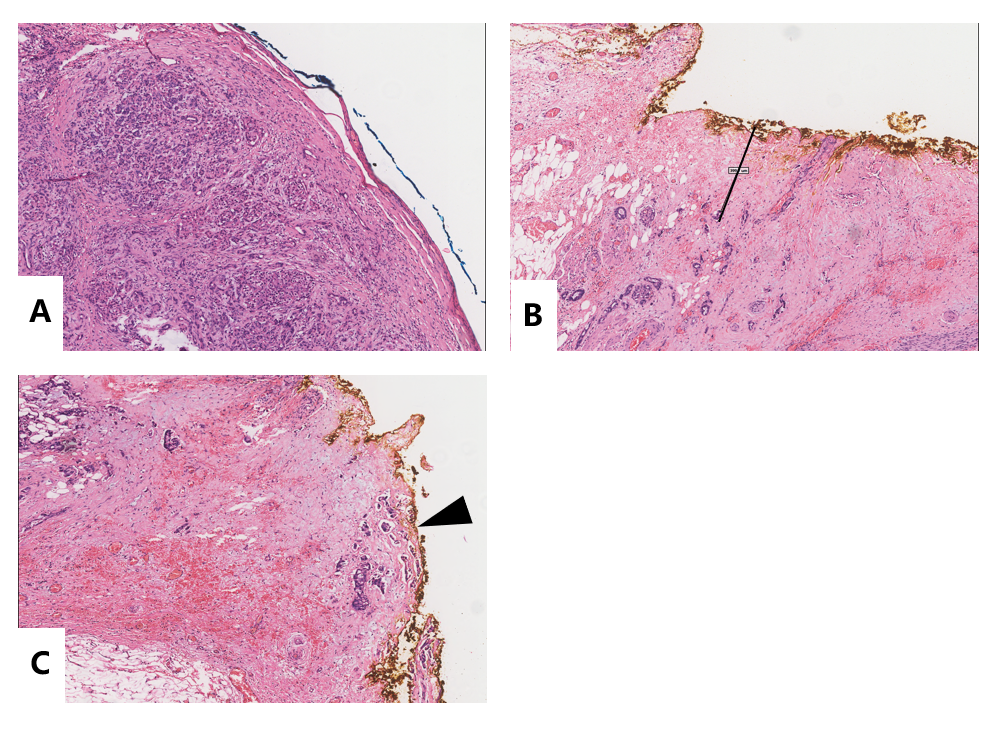
The entire specimen was sliced in 5-mm-thick sections, which resulted in 10–35 (average 24.5±6.7) formalin-fixed paraffin-embedded (FFPE) block for each specimen. Then, each FFPE block was cut in 4-mm-thick sections on whole-tissue glass slides measuring 7.8 × 5.4 cm2. These slides were scanned by the Hamamatsu S60 Whole Slide Scanner (Hamamatsu Photonics, Hamamatsu city, Japan) to obtain the DWMSIs with an average of 6.47 GB in file size [16]. The DWMSIs can also be observed by the NanoZoomer Digital Pathology (NDP) viewer2 version 2.7.25 (Figure 1), and the distance between the resection margins and the tumor cells can be measured precisely down to 0.01 mm on the screen (Supplementary Figure 1).
Classification and Defining of the R Status
The pathological reports on a detailed form were reassessed retrospectively. The slides were rechecked if the reports were not clearly depicted. According to the NCCN guidelines, the R status records for PD were comprised of the transection margin, the anterior surface, the posterior margin, the bile duct margin, the enteric margin, and the medial margin, which included the SMV (superior mesenteric vein)/PV (portal vein) resection margin and the SMA (superior mesenteric artery) resection margin. There were just three margins for DP. R1 was defined as one or more cancer cells within 1 mm of one or more surfaces or margins (R1<1 mm) or at the surface or margin (R1-directed). R0 was defined as >1 mm from any surface or margin (R0 >1 mm).
Variables Analyzed
For all the patients, the following demographic, clinical, and pathological variables, including sex, age, preoperative carbohydrate antigen (CA) 19-9, tumor location (head, neck, or uncinate process for PD; neck and body, or body and tail for DP), necrosis, perineural invasion, lymphovascular invasion, duodenal papilla invasion, tumor grade (G1/2 or G3/4), vascular resection. The TNM staging was also recorded using the 8th edition of the AJCC Cancer Staging Manual for Pancreatic Cancer. Resectability status was recorded according to the NCCN guideline for pancreatic adenocarcinoma (version 3. 2021).
Statistical Analysis
Categorical data were presented as percentage proportion, and continuous data were transformed into categorical data by the median value. For incomplete data, a dummy variable classified as “missing” was included in the analysis. To compare the differences in the categorical data between the two groups, the Fisher’s exact test or the c2 test was used as appropriate. All variables found to be statistically significant (P<0.1) on univariate analysis were subsequently included in a multivariate binary logistic regression model to determine the independent risk factors associated with R1 resection. For all the analyses, a two-tailed P<0.05 was considered as statistically significant. The analyses were performed using the SPSS version 25.0 (SPSS, Chicago, IL, USA).
{kind=link}