Lung cancer is one of the most common malignancies and remains the leading cause of cancer-related death worldwide (18). Pulmonary NET approximately accounts for 25% lung primary tumors, including TC (<1%), LCNEC (3%), AC (2%) and SCLC (20%) (2, 19). With the changes of environment, life habits, the profiles of lung cancer have changed gradually over the past decades (20). The incidence of SCLC is decreased but the incidence of NSCLC-NET is on the contrary, which gradually comes into view and brings more and more medical burden. Due to heterogeneity of NET, there is great difference of diagnosis, treatment and prognosis in SCLC and NSCLC-NET. Thus it is necessary to explore the difference between the two histological subtypes. Despite the prognostic model of SCLC has been reported, the prognostic nomogram for NSCLC-NET is still absent (20). Currently, predicting prognosis of NSCLC-NET mainly depends on TNM staging system. It has been well recognized that NSCLC-NET has obviously distinct prognosis with the other cancers. Therefore, the TNM staging system is not accurate enough to predict the prognosis of NSCLC-NET. To our knowledge, it is the first time that a prognostic nomogram has been constructed for guidance on prognosis of NSCLC-NET after operation.
In our study, we found that the incidence of NSCLC-NET had gradually increased but the incidence of SCLC had decreased since 1991. Moreover, female had higher incidence than male in NSCLC-NET, which meant NSCLC-NET may become the major subtype of pulmonary NET and bring bigger threat to female in the future. As for survival rate, patients with resected NSCLC-NET have significant better prognosis than SCLC. Further analysis demonstrated that TC had the highest 5 year survival rate, followed by AC, LCNEC and SCLC. The prognosis of LCNEC was similar to SCLC. It is worth noting, LCNEC is so similar to SCLC in its biological, clinical, and prognostic characteristics that LCNEC is excluded in some studies of large cell lung cancer (21, 22). According to WHO Classification Lung Tumors Classification [2015], LCNEC had been grouped with other neuroendocrine tumors (3).
In NSCLC-NET, patients receiving sleeve resection had the best prognosis but in SCLC, patients receiving segmental resection had the best prognosis. To some extent, sleeve and segmental resections conserve more lung function and is helpful for patients to recover as soon as possible, which may explain that patients with sleeve and segmental resection has better prognosis. The security and efficiency of sleeve resection has been validated in some studies (23). It is well recognized that smoking plays an important role in initiation and progression of lung cancer. Cigarette contains multiple carcinogenic substances (24). Smoking is also considered as a most common risk factor in development of chronic obstructed pulmonary disease(25). By analyzing smoking index, we found the higher the smoking index, the worse the prognosis in both SCLC and NSCLC-NET. It has been reported that SCLC has a strong association with cigarette smoking. About 95% SCLC patients have a history of heavy tobacco exposure (26).
The nomogram comprised six key factors, age, histological type, N stage, M stage, chemotherapy and surgery procedure. Age, N stage, and M stage are common prognostic factors in many cancers. Nomograms of many other cancers also include the three factors (27, 28). As for histological type, NSCLC-NET is an integrated cancer containing TA, AC, LCNEC. In fact, although the three cancers all derive from neuroendocrine cells and belong to non-small cells morphologically, they have distinct differentiation. TA, AC, and LCNEC are low-, intermediate- and high-grade tumors, respectively, which suggests that they have different malignant degrees (4). High-grade tumors commonly have stronger proliferation, invasion and metastasis, thus worse prognosis (29, 30). Many molecular makers associated with proliferation and epithelial-mesenchymal transformation have been developed to predict prognoses of cancer patients (31, 32). For advanced TA and AC, cytotoxic chemotherapeutic regimens are recommended. However, a standard chemotherapeutic regimen has not been established (8). Extended lobectomy has more chance to eliminate residues of tumor cells than lobectomy and reduces relapse and metastasis. Compared to pneumonectomy, extended lobectomy conserves more pulmonary function so that patients can recover faster and obtain higher quality of life (33). 1, 3, 5-year AUC of the nomogram were 0.873, 0.901, 0.875 and the C-index was higher than the conventionally used 8th edition AJCC staging system (0.87 vs 0.728, P < 0.001), indicating that the new nomogram had a strong discrimination. The calibration plot suggested that the predicting OS was highly consistent with the observed OS. In addition, compared to the 8th edition AJCC staging system, DCA demonstrated that the new nomogram had higher clinical usefulness. In 2020, Dong et al. constructed a predicting nomogram for OS of TC with 3, 5-year ROC of 0.824 and 0.812 (34). The nomogram for OS of AC developed by Chen et al. had 3-, 5-year AUC of 0.722, 0.737 (35). He et al. reported a predicting nomogram for OS of LCNEC with C-index of 0.75 (36). Thus, compared to the published nomograms, our nomogram not only integrated prediction for three subtypes of pulmonary NET but also had stronger predicting ability.
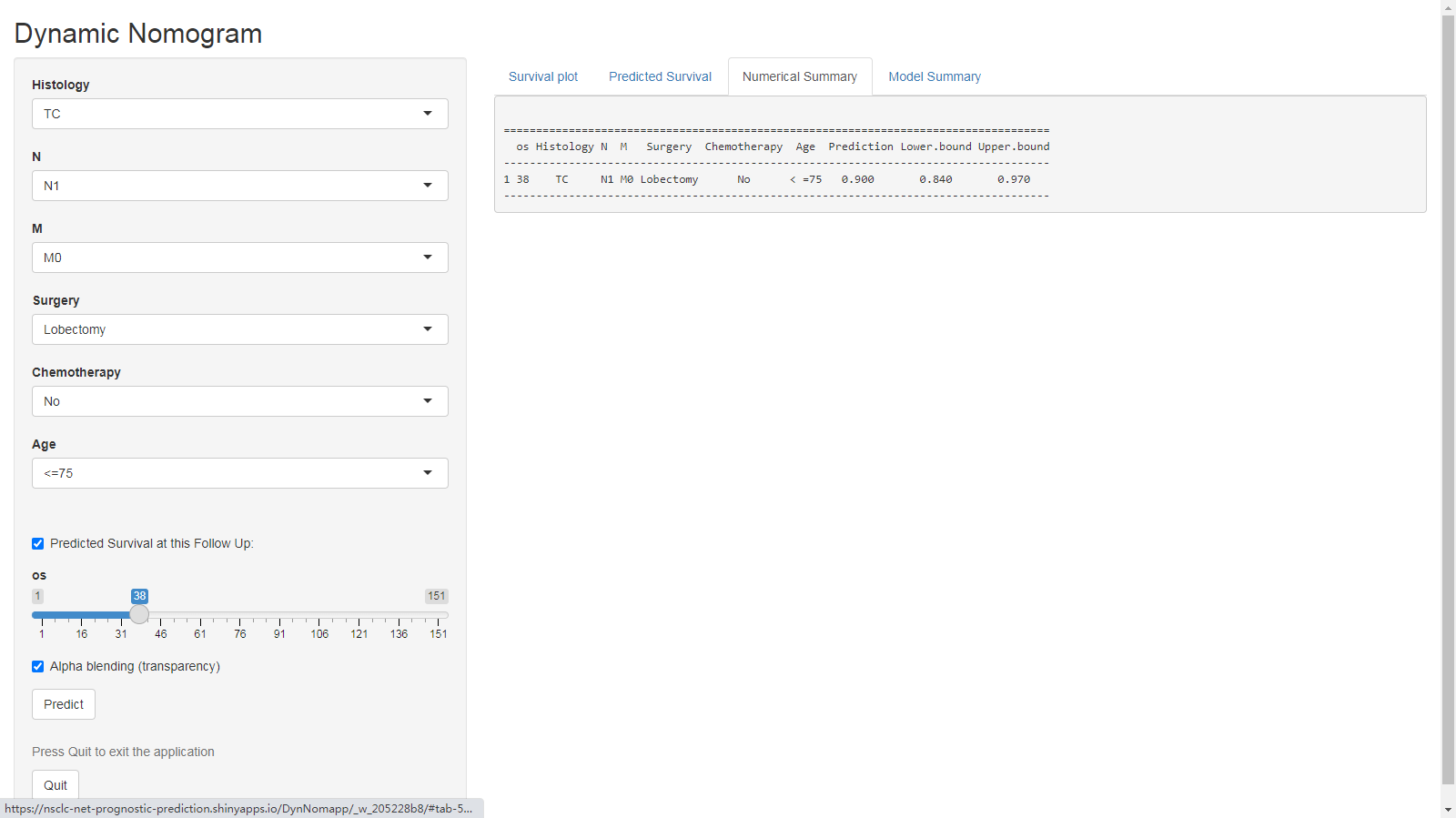
Our study has some advantages as follows. Firstly, our study was based on a large-scale population from the United States and validated by a Chinese cohort, which ensures reliability of our conclusion. Secondly, the study comprehensively compared SCLC and NSCLC-NET, including age-adjusted incidence, OS, LCSS, impacts of treatment strategies and smoking index on prognosis. Thirdly, it is first time that prognostic nomogram of NSCLC-NET has been established and evaluated by multiple methods such as C-index, ROC, calibration plot, DCA. Moreover, comparison with the 8th edition AJCC TNM staging system also demonstrated that the nomogram had better performance and certain clinical value. Last but not least, for convenient use for clinicians, we drew an online tool via ‘shiny’ package, which could easily show the predicting survival rate across time by inputting corresponding clinical features.
However, there are still some limitations in the study. First, it is a retrospective study so selection bias is difficult to avoid. Second, due to limitation of dataset, there are still some recognized factors affecting prognosis such as chronic obstructive pulmonary disease (COPD), drinking, specific chemotherapy regimen not included in the study. Last, the validation cohort from Shandong province hospital is not a multicenter data.
{kind=link}