Participants: This study recruited 38 patients with NNP ranging in age from 20 to 60 years who had been treated on an inpatient or outpatient basis at our institution. The details and procedures of the study were explained to the study participants, who all signed informed consent forms before being included in the study. The inclusion criteria were : ① male and female patients aged 20-60 years, VAS score for Neck skeletal muscle pain was greater than or equal to 3 points, ② chronic neck and surrounding tissue pain for more than 3 months, ③ patient had a diagnosis of at least one active trigger point on the neck, ④ reduced neck and shoulder range of motion due to pain, and ⑤ increased pain density caused by stress or lack of sleep. To improve validity, study subjects were included when all described conditions were satisfied.
In addition, NNP patients were excluded if they ① were younger than 20 years old or older than 60 years old, regardless of sex, ② were diagnosed with temporomandibular arthritis or fibromyalgia,③had uncontrollable pain or other discomfort during treatment, ④ had excessive muscle tension or mental anxiety during injection treatment or severe swelling and bleeding after injection treatment, ⑤ had acute pain in spine (< three months) ,radiculopathy and other spine related conditions.
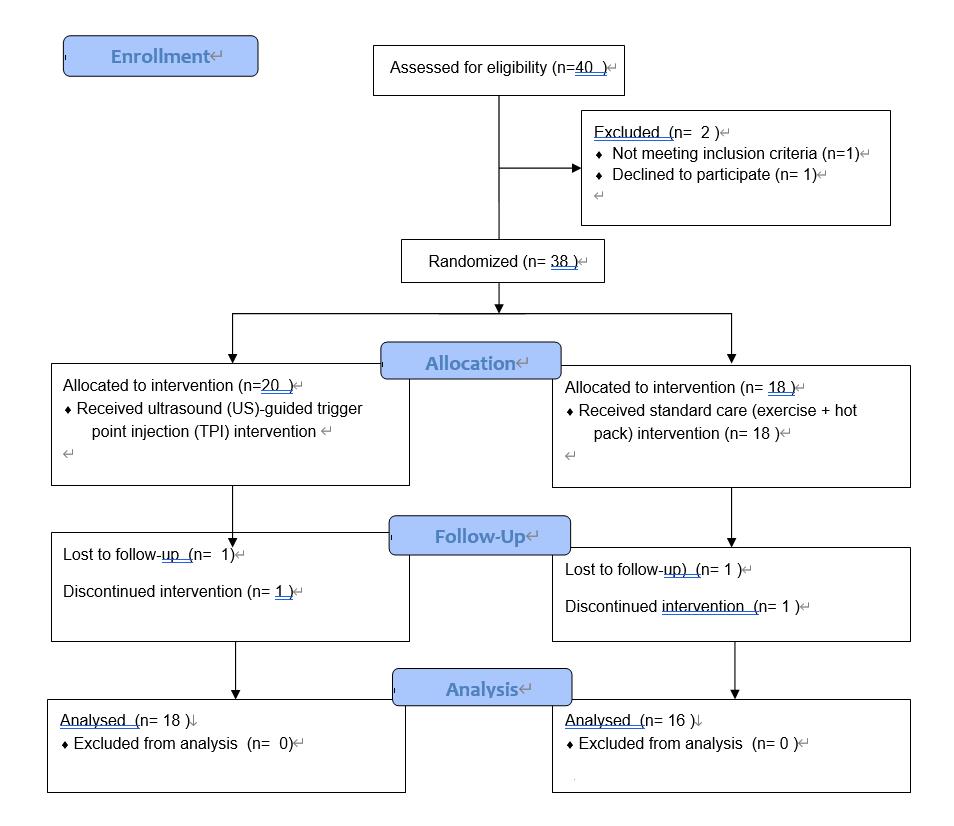
Patients were randomly assigned into the control group (n=18) or ultrasound-guided TPI group (n=20) by using computer-generated randomization allocation software, Sex was not taken into account during the randomization. The allocation procedure of the participants is presented in the Flow Chart.
Interventions:
Patients with spine, nerve roots or other spinal-related diseases were ruled out by using magnetic resonance imaging (MRI). The therapist used a combination of physical examination and ultrasound examination to locate and mark the MTrPs of the upper trapezius muscle (Figure 1). All the therapists, evaluators and statisticians were blinded to the participants data.
For participants in the TPI group, a single dose of 3 ml of 0.5% lidocaine was injected into each trigger points in all affected muscles under ultrasound guidance once a week for 3 weeks, Patients were asked to sit in a straight, upright position throughout the treatment. The injection was administered with a 25-gauge, 1.25-inch long needle with the tip perpendicular to the skin, under ultrasound guidance, a needle was inserted into the upper trapezius muscle until the positions of MTrPs were accurately determined. After the injection, the needle was moved back and forth. The same point was needled repeatedly, and the tip of the needle was withdrawn from the muscle[21].
The participants in the control group received conventional physical therapy treatment (heat therapy and exercise). Heat therapy was applied directly over the trapezius muscle of participants for 15 minutes. Then, they performed exercises under the supervision and assistance of an experienced physiotherapist. Each exercise was repeated 10 times for 5-10 s. The treatment was repeated every other day for a total of three weeks[22].
Outcome measurements:
The visual analog scale (VAS) is a sensitive and comparable method used to measure general pain intensity. The specific method is as follows: a 10 cm horizontal line is drawn on paper, one end of the horizontal line is 0, indicating no pain, the other end is 10, indicating severe pain, and the middle part indicates varying degrees of pain. The participant is asked to draw a mark on the horizontal line according to their self-perceived degree of pain[23].
The Neck Disability Index (NDI) was used to evaluate cervical spine function. The evaluation form included a total of 10 questions concerning neck pain-related symptoms (pain intensity, headache, concentration and sleep) and activities of daily living (personal care, lifting heavy objects, reading, working, driving and entertaining). The patient answered truthfully according to his own situation. The higher the score, the more severe the dysfunction is: with zero indicating no disability and five indicating complete disability (0= no disability, 5= complete disability)[24].
A Sonosite M-Turbo US system (FUJIFILM Sonosite Inc., Bothell, WA, USA) with a transducer cover and sterile coupling gel was used to locate the upper trapezius trigger points. Scanning was performed using a 13-6 MHz linear transducer. Normally, there are some grayscale degree and pattern changes in areas with MTrPs that appear as focal hypoechoic and heterogeneous echotexture regions. Therefore, we used musculoskeletal US to locate, guide and administer TPI for NNP, and evaluated the effect of myofascial structural changes before and after treatment[25, 26].
sEMG analysis was performed with a device (Shanghai Nuocheng Electric Co., LTD) on the upper part of the trapezius muscle bilaterally. The motor unit activity in EMG recordings ranges from 70-90 Hz, the time base for recording was 1000 ms, the scanning speed was 3 s/D, and the amplification was 80 μV/D during maximal contraction of muscle. A pair of the standard bipolar electrodes was placed on the surface of the skin over the muscle belly. The sEMG recordings were performed during maximal voluntary contraction of-the trapezius muscle for 5 s and repeated for 3 times to measure the amplitude [27].
The soft tissue stiffness of each point was assessed by sonoelastography. An musculoskeletal ultrasound system (SuperSonic Imagine Aixplorer, France) with an SL15-4 linear transducer and frequency of 4-15 MHz was used to perform resting mode sonoelastography in the sitting position. To perform a comprehensively inspect the muscles at the mark, the detection depth was set to 2~3 cm[28].
Infrared thermography (TMT-9000P, Hangzhou Xinhan Photoelectric Technology Co., LTD.) was used to measure skin temperature changes over the upper trapezius muscle in our special infrared shielding room. The patient was instructed to sit and rest for 5-10 minutes before the test, and then positioned 2.5 m from the infrared camera for ITI according to the prescribed standard position. The infrared thermal images taken were analyzed by software, and the difference in body surface temperature was distinguished by the difference in color scale[29].
Statistical analyses:
The total sample size was calculated to be 40 (20 in each group) with a 10% acceptable drop-out rate by using G-POWER software. The descriptive statistics are shown as the calculated mean and standard deviation. One-way ANOVA was used to perform intergroup comparisons of the baseline data. T-tests were used to compare the effect before and after treatment in terms of VAS score, NDI, sonoelastography, EMG and infrared thermography data in the two groups. Similarly, T-tests were used to compare results between the two groups. All statistical analyses were performed with SPSS (version 23, IBM Corp., Armonk, NY, USA). All tests of statistical significance were interpreted with a criterion of p<0.05.
{kind=link}