It is consistently challenging for clinicians to make accurate diagnoses regarding the level of dental pulp inflammation[4]. As new biological materials are developed, vital pulp therapies are increasingly used, which can increase the fracture resistance and long-time survival of teeth[31]. However, there is currently no accurate diagnostic tool for guiding dental pulp treatment; this shortcoming is an important cause of failure in vital pulp therapy[32]. Since histological examinations show that the extent of inflammation is not correlated with clinical manifestation, traditional diagnostic approaches based on symptoms or electrical/thermal pulp tests, require improvement[9, 33].
During inflammation, cells in human dental pulp, including odontoblasts, macrophages, vascular endothelial cells, precursor cells and other cells that can activate the immune system, secrete large amounts of cytokines, chemokines and neuropeptides, which have been reported to play critical roles in inflammation[34, 35]. Sivakami et al found that the levels of IL-6 and the cytokine interleukin-1β (IL-1β) were clearly increased in saliva during pulpal and periapical inflammation[36]. An analysis of cytokines in pupal blood revealed that the levels of IL-8 were significantly higher in irreversible pulpitis than in caries-exposed pulp[37]. Several cytokines have been reported to be candidate diagnostic markers of pulpal inflammation[23, 38]. However, to the best of our knowledge, no biomarkers with high degrees of accuracy have yet been used in clinical examination to diagnose early pulpitis.
Research involving microarray analysis is rapidly expanding due to the rapid development of transcriptomic studies, resulting in an increasing understanding of the biological mechanisms underlying oral diseases[39]. Through the integration of several similar datasets, we can generate comprehensive expression profiles to identify key genes that can serve as biomarkers of pulpitis diagnosis and prognosis.
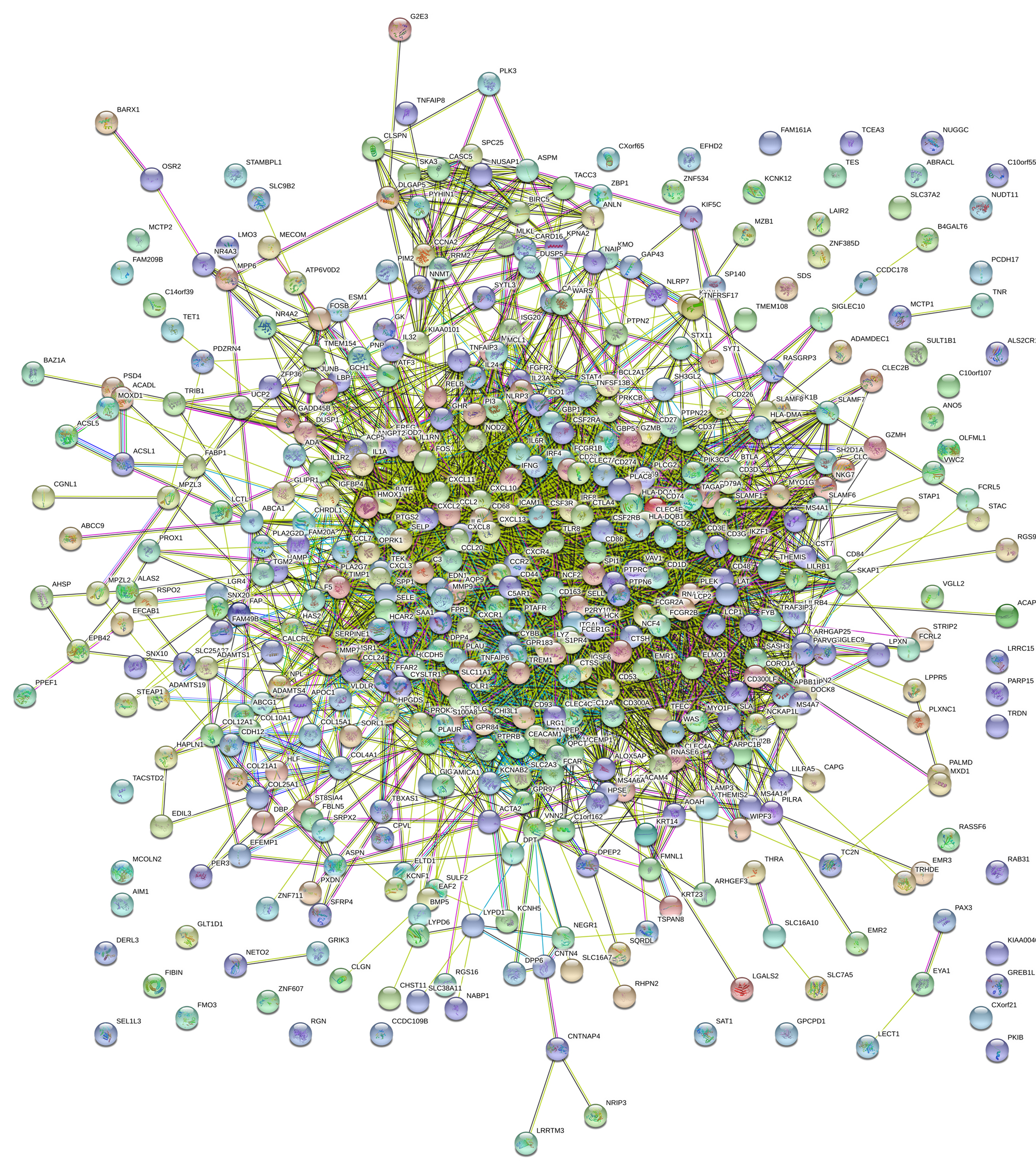
In the current study, expression data of pulpitis tissue from the GEO database were integrated and then used to identify the underlying characteristics of DEGs and candidate biomarkers for diagnosing the inflammation level of dental pulp. Li et al reported DEGs and enrichment results obtained by analysing data in the GSE77459 dataset[40]. In contrast, we extracted data from GSE77459 and GSE92681 and integrated the mRNA expression data to remove batch effects and improve the quality of the data. Batch effects are the effects of technical differences unrelated to biological variation that are caused by the processing and measurement of samples in different batches, such as experiments that are conducted at different times or with different methods by different technicians[41]. The ComBat function and sva function of the SVA package that we used for data processing are useful for removing both known batch effects and other potential latent sources of variation[28]. After data processing, GO and KEGG pathway analyses were performed. The enrichment results revealed that the identified DEGs are involved in processes associated with dental pulp inflammation. Ten hub genes of pulpitis (PTPRC, TLR8, CD86, IL6, CCL2, MMP9, CXCL8, SPI1, ICAM1 and LCP2) were identified from the PPI network, and the possible mechanisms by which hub genes induce inflammation were investigated by GSEA and found to involve the complement system, IL6/JAK/STAT3 signalling pathway and inflammatory response pathways. Enriched KEGG pathways identified in both the present study and that of Li et al[40] were cytokine-cytokine receptor interaction and chemokine signalling pathway, and hub genes common to the two studies were IL6, CXCL8, PTPRC, CCL2 and ICAM1.
PTPRC encodes protein tyrosine phosphatase (PTP), a signalling molecule that regulates various kinds of cellular processes and plays a critical role in the immune system. PTPRC can negatively regulate cytokine receptor signalling by suppressing the JAK signalling pathway[42]. PTPRC is expressed at low levels in normal dental pulp tissue[43] but at high levels in pulpitis tissue, as described above. CD86 is a receptor that commonly participates in T-lymphocyte proliferation and IL-2 production, acting as a negative regulator for the immune system[44]. Miyuki Azuma et al studied immune responses in mouse dental pulp and found that expression of CD86 was enhanced in dental pulp after cusp trimming but disappeared within 2 h, with CD86 migrating into the regional lymph nodes at 24 h after acid treatment[45]. Chemokines activate and support the process of dental pulp inflammation. Accordingly, increased expression of CCL2 has been observed in chronic periapical lesions, indicating an association between chemokines and dental pulp inflammation[46, 47]. In addition, IL6, MMP9, TLR8, CXCL8, and ICAM1 have been reported to be associated with immunity and inflammation in dental pulp[1, 17, 48–51]. The above hub genes may play critical roles in pulp inflammation and therefore be potential biomarkers for use in pulpitis diagnosis. However, associations of LCP2 and SPI1 with pulpitis have not been reported previously.
During the treatment of deep caries and traumatic exposure of dental pulp, it is essential to assess whether the pulp inflammation is reversible. It has been reported that inflamed pulp tissue might produce some biomarkers that are secrete to the external environment[13, 14], making tests of dental pulp blood and dental fluid in pulpitis possible. Johannes et al[17] used heparinized 10-mL microcapillary tubes to collect pulp blood samples when the dental pulp was exposed during caries removal. The MMP9 levels from blood sample of irreversible pulpitis were highly increased compared with those from blood samples of asymptomatic or reversible pulpitis teeth. In addition, dental fluid contained within dentinal tubules has been proposed to be potentially useful as a biomarker of different stages of pulpitis. By detecting the dental fluid in tooth cavities using polyvinylidene difluoride membrane, Brizuela et al[18] found that the biomarkers of fibroblast growth factors acid (FGF-acid), interleukin-1α (IL-1α), IL-6, and tissue inhibitor of metalloproteinases 1 (TIMP-1) may collectively be useful for molecular diagnostics in pulpitis. Due to its advantages of ease-of-use and non-invasiveness, the dental fluid test is a promising method for the molecular diagnosis of pulpitis. However, dental pulp blood analysis might more accurately reflect the pathophysiologic conditions of dental pulp in inflammation[52]. The goal is to develop a low-cost, non-invasive, chair-side rapid method of pulpitis diagnosis. It has been reported that a rapid chair-side test of MMP8 in gingival crevicular fluid can be used to distinguish periodontitis from gingivitis and healthy gingiva[53].
However, in addition to the challenges of sample collection, many difficulties in the analysis and application of biomarkers need to be overcome. Much progress remains to be made in developing an effective method for molecular diagnosis in the clinical setting, which is the one of the limitations of the current study. In addition, due to the paucity of available datasets of pulpitis in the GEO database, the sample size in this study was limited. We will increase the sample size in a future study if additional datasets can be retrieved from the database.
{kind=link}