The present study was based on data from a region with high incidence of SARS-CoV-2 infection during the initial wave of COVID-19. To the best of our knowledge, it comprises the largest German cohort of COVID-19 patients with detailed and comprehensive clinical data in individual patients. The study demonstrated the great importance of patients’ treatment limitations (PTL) for mortality from this disease. Between 33 and 42% of patients had at least one limitation regarding rejection of admission to ICU, or intubation, or cardiopulmonary resuscitation. Limitations were associated with age, dementia, the CCI and renal function in terms of eGFR. Their association with mortality was strong and robust, and independent from other predictors such as the burden from comorbidities, oxygen saturation by pulse oximetry, renal function, CRP and neutrophil number upon hospital admission. In summary, PTL appeared as a further, comprehensive, previously unrecognized determinant of death from COVID-19 that added to or partially replaced known predictors. This novel finding might be useful for a more detailed understanding of the mortality from COVID-19 including the large variations across countries and locations.
With regard to age and sex, the present population was similar to cohorts of SARS-CoV-2 patients from Germany [3, 20] showing a median age of 72 and 73 years, respectively, and a slightly higher percentage of males (51.8 and 51.5%, respectively). In line with these studies and findings in other European regions and countries, [4, 5, 10, 11] we observed that most patients had a least one major comorbidity. Among these, systemic hypertension, left-heart failure, renal disease, diabetes and malignant disease were most frequent. Interestingly, in the study by Nachtigall and co-workers [3] the proportion of patients with at least one comorbidity was only about half as large as in our cohort. Differences in comorbidities between studies were also reflected in the CCI. When computed without age, about 53% of patients of our cohort showed a CCI of ≥2, and when including age, this percentage raised to about 79%, compared to 55% in the study by Karagiannidis and co-workers. [20] The relevance of comorbidities and age and their differences between populations was also evident for treatment limitations. When not taking into account age, the median CCI was 1 in patients without limitations and 3 in patients with at least one limitation but when computing the CCI with age, the respective median values were 1 and 7.
In the total population of hospitalized patients, mortality was 27.2%, similar to that of the prospective observational UK cohort study [4] but higher than in German cohorts (22% and 16.6%), [3, 20] although the distributions of age and sex in our study and the previous two studies from Germany were not much different. [3, 20] In the PRECOVID study from Spain, [5] 771 of 3,641 patients (21%) died irrespective of hospitalization. Thus, mortality was in the upper range in our cohort, and this might have been related to the large frequency of treatment limitations as underlined by Figure 1.
An important recent observation was that in patients admitted to hospital with COVID-19, outcomes were better predicted by frailty than by age or comorbidity. [21] These factors are closely related to treatment limitations that might affect mortality risk by limiting the scope of interventions. Such limitations are well known as DNR and DNI statements regarding resuscitation and intubation, respectively. We added the acceptance of ICU treatment as a third, more general limitation that turned out to be informative. It appears surprising that these limitations have not been explicitly addressed in COVID-19 patients, even more, as we found the proportion of patients with treatment limitations to be one third and more. Clinical experience shows that decisions on treatment limitations are founded in objective medical factors including age and comorbidities, [22] but also personal attitudes and preferences, both on the patients’ or relatives’ and the physicians’ side. The complex interplay between these factors is reflected in changes occurring after consultation and discussion, [22] and it is probably impossible to disentangle these factors retrospectively in detail. Irrespective of this, major objective determinants could be identified in our study (Table 1 A/B, Table 2). In patients with treatment limitations, mortality rate reached 85% in the subgroup of ICU-patients with mechanical ventilation. This high mortality corresponds to the high rate of DNR in this population. It might also be related to a higher use of opioids as previously reported in patients with DNI/DNR limitations. [23] In contrast, overall mortality rate appeared low (12%) in patients without any treatment limitation. Future studies might show whether these limitations explain part of the variation of mortality from COVID-19 within and across countries.
As independent predictors of treatment limitations, we found age, dementia, cardiovascular disease, CCI and eGFR being <55 ml/min, a result which appears plausible from both the patients’ and the physicians’ perspective. Regarding the accuracy of prediction, the contribution of these objective measures to the final PTL was 80% and more. The remaining 20% obviously comprised other factors including subjective factors. In line with proposals made previously, [17] this observation could be helpful in understanding decision making in a severe life-threatening disease such as COVID-19. The most remarkable finding was that treatment limitations were related to mortality beyond known prognostic factors by integrating some though not all of these into a comprehensive indicator (see Figure 2). This suggests that they constitute an individual factor having considerable impact on the prognosis in COVID-19.
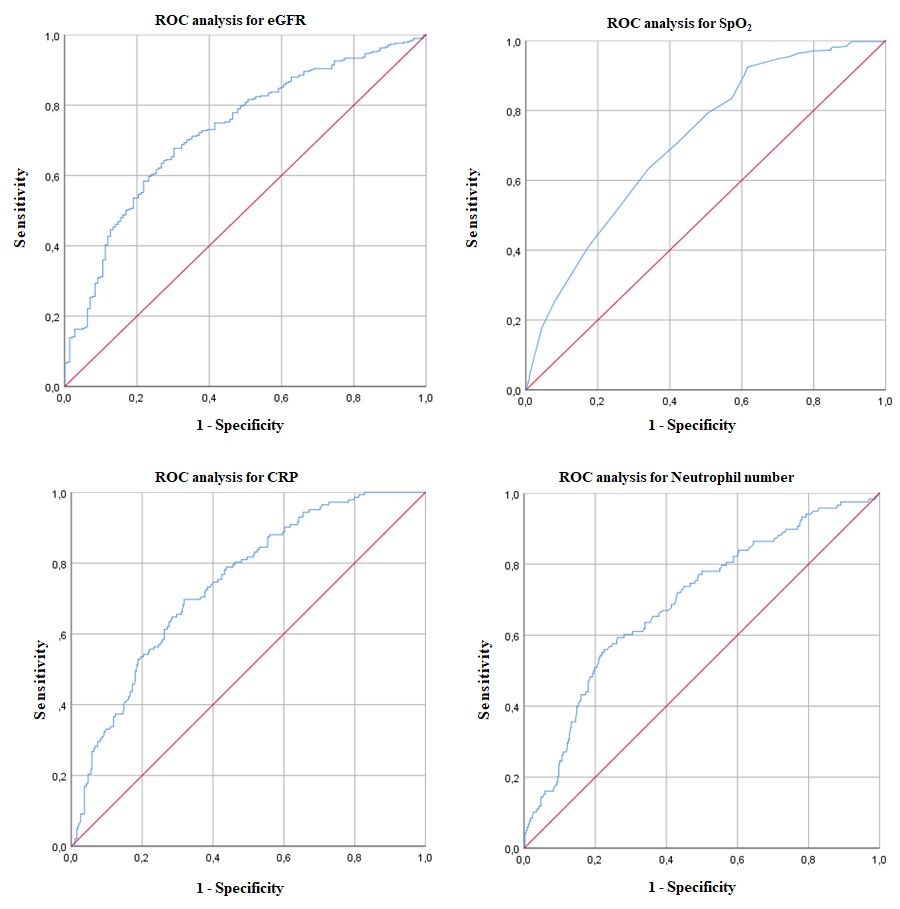
In line with the literature, we found age, blood pressure, SpO2, comorbidities, hemoglobin, leucocyte, lymphocyte and neutrophil numbers, creatinine, eGFR, LDH, CRP and IL-6 to be predictive for mortality. [5, 10-12, 16, 24, 25] ROC analyses (see supplement, Figure S1) yielded cut-off values regarding neutrophil number ≥5 G/l, CRP level >7 mg/l, eGFR <55 ml/min and SpO2 <93% which were identified as independent risk factors for mortality in multivariate analyses. Noteworthy enough, the predictive value of eGFR upon admission was superior to that of the corresponding creatinine value or the diagnosis of a preexisting renal disease. The deleterious effect of renal impairment is probably linked to endothelial dysfunction and increased cardiovascular risk, both of which affect the outcome of COVID-19. [26] In the current analysis, eGFR appeared of particular interest, as it was a strong predictor of both, treatment limitations and mortality.
Limitations
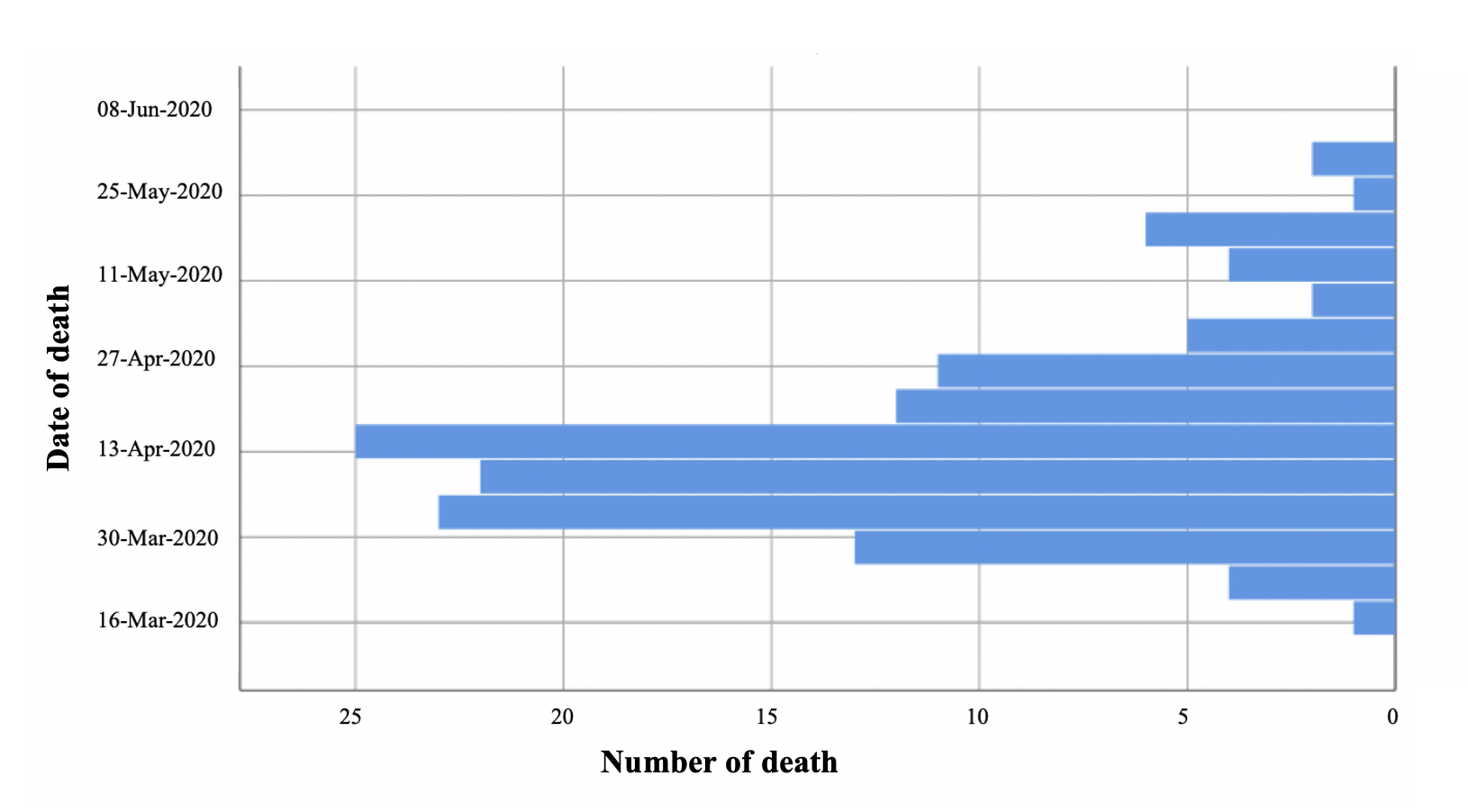
The present analysis comprised only a limited number of patients with SARS-CoV-2 infection compared to large studies reported in the literature. [4, 5, 10, 20, 27] On the other hand, we performed a comprehensive, standardized assessment of patients allowing the evaluation of clinical management and risk factors in a hotspot region. We restricted our analysis to the initial wave of COVID-10 with its sharp rise and decline (see supplemental Figure S2), as this provided high case numbers and fairly homogeneous conditions. The prognostic values of markers such cardiac troponin [16] and d-dimer [25, 28] could not be evaluated in the total population, because the respective kits differed between locations and were difficult to compare; when analyzing the Rosenheim data alone, troponin was significantly related to mortality, as expected (data not shown). Furthermore, detailed information on body mass index (BMI) and smoking status, which have been identified as additional prognostic markers in large cohorts with COVID-19, [4, 29, 30] was not consistently available from the files. Moreover, we did not have detailed information on the processes by which treatment limitations were determined in each single case, and relied on the well-established, routine procedure involving patients, relatives and treating physicians.
{kind=link}
{kind=link}