In 2020, China hopes that national malaria elimination will become a real possibility based on effective control measures [4]. Although no indigenous malaria case has been reported in China since 2017, the imported malaria is becoming a serious obstacle for malaria elimination. If China plans to achieve the stated goals on schedule, continuous surveillance of the imported malaria is an essential measure. As an important city of Central China, Wuhan has a population of 11.08 million. Meanwhile, it faces similar problems: The imported malaria cases increased annually accompanied by the disappearance of indigenous malaria cases since 2013 [5]. Thus, it is very necessary to monitor the epidemic status of imported malaria in China including Wuhan. Furthermore, identification of the malaria parasite species with timely and effective method could provide valuable information for developing suitable clinical treatment.
In current study, of the 243 P. falciparum cases identified by microscopy, one case actually was proved to be infected with P. falciparum plus P. ovalis later by both molecular tests. Two microscopy positive P. vivax cases were also proved to actually infect with P. vivax plus P. ovalis. Likewise, two patients with single P. ovalis infection by microscopy were proved as P. ovalis plus P. falciparum infection by nested PCR. In the previous studies, P. ovale was also frequently reported involved in mixed infection with other Plasmodium species [17, 43, 44]. These results proved the limitation of microscopy in identification of mixed infection and the highly specialized requirement for observers [45]. The identification of P. ovale curtisi and P. ovale wallikeri in total 20 single P. ovalis infection cases, which were failed to be distinguished by microscopy, also evidenced the advantages of molecular tools in species identification. Their diagnosis will offer a clue for the precise treatment of malaria patients. Subsequently, nested PCR also proved 6 cases as P. falciparum infection, which were consist of 5 microscopy negative but RDT positive cases and even one double-negative case. This was probably because parasitaemia was too low to be observed for these cases. As reported previous studies [46, 47], microscopy has a sensitivity of 50 ~ 500 parasites/µl in Plasmodium detection, but the threshold, 50 parasites/µl was rarely obtained unless under optimum conditions. This means that, it is actually difficult for observer to accurately find out the species with relative low parasitemia, especially in mixed infection.
In the analysis of sensitivity, specificity, PPV and NPV, nested PCR-based detection was chosen as the reference standard. Actually, nested PCR was commonly selected as a reference method [48, 49]. By comparing to nested PCR, microscopy (96.77%) showed highly similar sensitivity with real-time PCR (96.37%) in P. falciparum identification. However, the specificity of microscopy was only 91.67%, lower than the 100% in rea1-time PCR detection. By designing complementary probe to target gene sequence, Taqman probe is another guarantee besides primers to enhance the specificity and avoid the false positive results [35]. The NPV for P. falciparum detection was about 85% in both microscopy and real-time PCR detection, indicating relative high false negative rate about 15% appeared in these two methods. A false negative rate as high as 19.4% for microscopy assay was reported in other study [50], indicating the persistent limitation of microscopy. For P. ovalis, the sensitivity (88.00%) in microscopic identification was relative low and NPV for P. ovalis was 98.91%. Two of the 3 P. ovalis cases that failed to be detected out by microscopy were involved in P. ovalis plus P. vivax mixed infection. This may due to the similar morphology between P. ovale with P. vivax [10], as a result, the species with relative lower parasitemia may be hidden. Four indexes (Table 4) in real-time PCR detection were all 100% in P. vivax, P. malariae and P. ovalis detection, revealing the high consistency between two molecular tools in these three species identification. P. malariae could be accurately diagnosed by all the three methods. This may be attributed by only 6 P. malariae cases were involved in the study. The primers of real-time PCR used in this study have been used in several previous studies [32, 51]. But it is reported that different templates amplification simultaneous was difficult and the primers preferred to amplify species with higher parasitemia as result of competition for the shared primers (Plasmo1 and Plasmo2). In present data, 7 cases out of the total 9 nested PCR positive patients failed to be identified by real-time PCR. Actually, all had low parasitemia and the remained two were involved in mixed infection. Similar phenomena also reported in previous studies [52, 53]. As we know, false negative result means a person with Plasmodium infection failed to be diagnosed. This could cause misdiagnosis, delay treatment of malaria and even lead to a life-threatening problem, especially for P. falciparum infection. Beyond the individual damage, false negative patients may also spread malaria and produce resistance to antimalarial drugs without correct treatment guided by exact diagnosis [50].
Although nested PCR showed the highest sensitivity and real-time PCR has the best specificity, the role of microscopy and RDT is still not substituted. Because conduct of the two molecular methods is relied on DNA extraction of blood samples. Once errors happened during this program, the false negative would probably present. For example, in a previous study, there were 10 malaria cases failed to be identified by molecular methods due to the problems in nucleic acid extraction until reasons were found out by repeated experiments [54]. Therefore, the combining use of the four methods is quite necessary and highly recommended. Both microscopy and RDT can offer the preliminary result and suggest further diagnostic direction. Based on the valuable information, the Plasmodium species can be confirmed by molecular methods easily including nested PCR and real-time PCR.
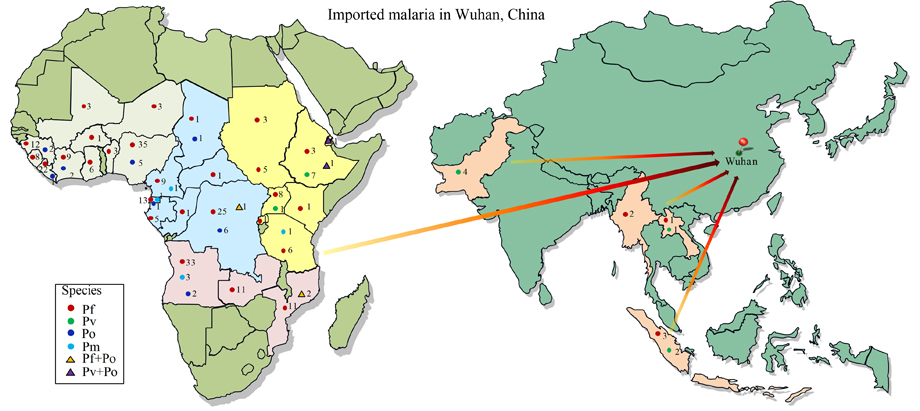
The origin of patients was basically consistent with a previous report referring to epidemiologic features of imported malaria in the whole China [55]. In these epidemic regions of Africa and SEA, the natural environment, healthcare and situation of economic development may be primary influences on malaria infection. Chinese people overseas especially those didn’t long-term inhabit in epidemic areas usually lacked adaptive immunity and related awareness to local Plasmodium infection [55]. Additionally, there were frequently asymptomatic patients existing [56]. These remind us that workers returned from these areas particularly West Africa, Central Africa, and Southern Africa should be recommended to accept malaria diagnosis. As the dominating malaria species, P. falciparum was similar to other study [50]. Therefore, prevention and treatment against P. falciparum should be highly considered in Wuhan. By the year elapsed, the Plasmodium species leading to imported malaria were becoming diversity just as the situation in another region of China, Shandong province [54]. The increase of imported P. vivax and P. ovalis cases may cause the re-introduction of malaria in those regions without cases [57, 58]. P. malariae could maintain in human for many years and keep infectivity to its vector at a really low parasitemia [59]. Thus, more attention should be payed on this increasing diversity. The sharp decrease of imported malaria cases in 2017 was a good sign indicating the performance of malaria control. However, the cases raised again in 2018, warning us the great challenging for complete elimination of Plasmodium infection worldwide, even in China.
{kind=link}