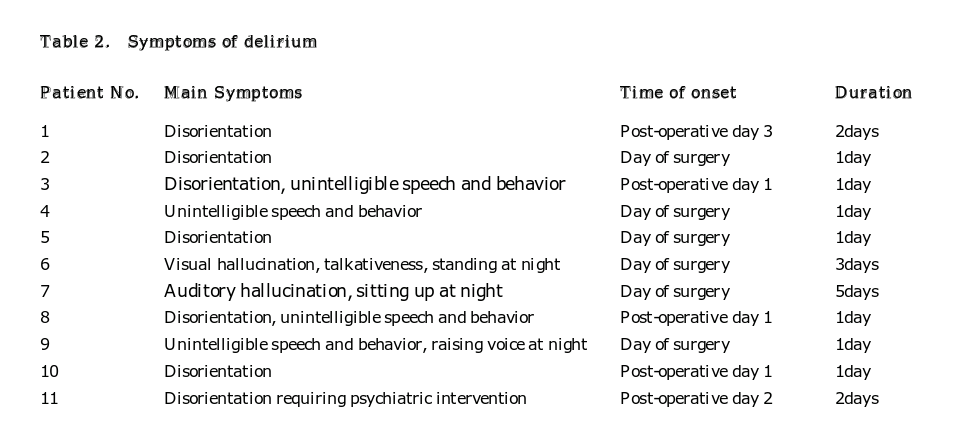
The presence of delirium increases the risk of developing dementia later in life.[24] Although generally a temporal condition presenting with psychiatric symptoms, delirium can lead to decreased quality of life and reduced ability to perform routine activities; therefore, its prevention and treatment are important, especially in elective surgery.
Delirium is generally induced by organic brain damage, systemic diseases, and pharmacological factors. The causes of delirium are often difficult to identify, and multiple factors are believed to be involved in its pathogenesis. The most well known risk factors are history of delirium (odds ratio, 4.1), advanced age (≥70 years) (odds ratio, 3.2), and pre-existing cognitive dysfunction before surgery (odds ratio, 2.2).[25] Other reported risk factors for delirium include low Hb or Ht, malnutrition, and dehydration, by causing low blood pressure and metabolic imbalance leading to hypoxic brain injury.[11, 26] It was also reported that the risk of delirium increased 1.15-fold per year increase in age.[9] As the number of elderly patients undergoing TKA has increased in recent years, attention to incidence of post-operative delirium is warranted in clinical practice, as this affects time until ambulation and duration of hospital stay.[14] This study consisted of patients with a higher average age compared to previous studies, and also included a larger number of bilateral TKA.[9, 14] In this study, the incidence of post-operative delirium after TKA was 6.5%, similar to previous reports, and no difference was observed between unilateral and bilateral TKA patients, despite bilateral TKA consisting of longer surgery time and increased peri-operative blood loss.
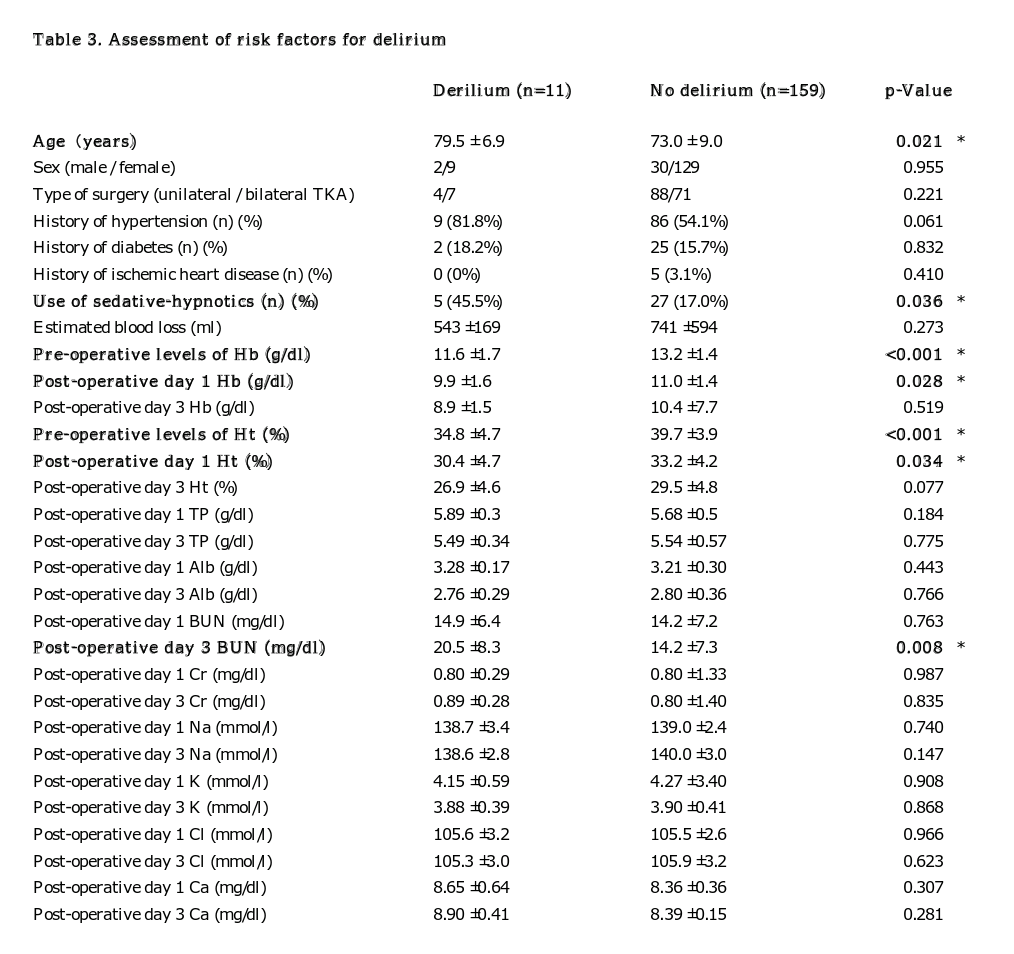
The pathogenesis of delirium is complex and multifactorial, and the utilization of multivariate analysis is a useful approach for identifying significant risk factors. Multivariate analysis of risk factors for post-operative delirium after TKA identified the use of sedative-hypnotics and a pre-operative Hb level of <11.1 g/dL as independent risk factors. The use of sedative-hypnotics increased the risk of delirium by more than 4 times. Age, Hb/Ht level on post-operative day 1, and BUN level on post-operative day 3 showed significant differences in the univariate analysis but not in the multivariate analysis. Given that the Hb/Ht and BUN levels are associated with dehydration and anemia, further analysis is required to assess their true association with delirium.
In recent years, there have been reports that benzodiazepine receptor agonists (benzodiazepines and non-benzodiazepines) may cause cognitive decline, mental dependence, delirium, and muscle relaxation, with increased risks of falls and proximal femoral fractures.[15, 27, 28] New insomnia drugs, such as ramelteon and suvorexant, act selectively on the pineal and hypothalamic receptors (melatonin receptor and orexin receptor), respectively, potentially reducing the risk of delirium. Furthermore, Hatta et al. reported in a randomized clinical trial, that ramelteon and suvorexant even showed suppressive effects against delirium.[29, 30] Therefore if possible, switching from benzodiazepine receptor agonists to these drugs prior to surgery may have a preventative effect for pre-operative elderly patients against delirium.
There has been a growing interest in the role of anemia in cognition among older adults. Recent systematic review and meta-analysis showed significant positive association between anemia and global cognitive decline, reduced executive function, and the incidence of dementia.[19, 31] A recent report suggested anemia as an independent risk factor for delirium in hospitalized older patients along with dementia in a small cohort of 190 patients.[32] However, in a more recent multicenter study, no evidence of association was found between anemia and cognitive impairment.[33]
Tranexamic acid has been shown to decrease intra-operative blood loss and the need for overall blood transfusion in knee and hip arthroplasties, and its efficacy and safety has been evaluated in a meta-analysis.[34-36] However, pre-operative anemia remains a risk-factor for blood transfusion despite tranexamic acid administration, and attempts to minimize post-operative Hb decrease have not been sufficient to compensate for low pre-operative Hb.[37] Furthermore, pre-operative blood transfusion remains controversial, with reports of multiple complication associated with pre-operative blood transfusion in hip arthroplasty.[38]
Oral iron supplement has not been proven to be beneficial, due to its low absorption rate and gastrointestinal side-effects.[39] Intravenous iron therapy on the other hand is a more effective method with fewer side effects. It reduced the rate of transfusion and length of hospital stay, but there is no conclusive evidence at present to suggest that correcting pre-operative anemia results in reduced risk of delirium post-operatively.[40]
Although no definitive preventative measures for delirium exist, its multi-factorial nature suggests that for elderly patients with either low Hb or sedative-hypnotics, particular consideration is necessary to reduce other potential risk factors such as peri-operative bleeding and dehydration. Current hospital practice involves minimizing blood loss intra-operatively by administering tranexamic acid and avoiding dehydration by administration of intravenous fluids peri-operatively. We encourage early rehabilitation and gait exercise to prevent prolonged bed stay to reduce post-operative complications. However, no specific measures had been taken to identify and reduce the risks of delirium. As a result, previous pre-operative assessment included rigorous medical assessment, but lacked cognitive assessment and did not take into account the use of pre-operative benzodiazepine receptors. Taking into account the findings from this study, we are developing a new hospital protocol, to be particularly cautious in patients with Hb <11.1g/dl, and explaining the risks of delirium to patients and their family. Furthermore, we are screening for patients who are taking benzodiazepine receptor agonists, and where possible, switching them to alternative sedative-hypnotics such as melatonin and orexin receptors prior to surgery. In addition, administration of benzodiazepine receptor agonists are avoided post-operatively.
There were several limitations in this study. First, the study design was retrospective, and therefore the details of delirium could only be assessed based on the existing medical records. More importantly, pre-operative cognitive function was not assessed, which is an indicator of post-operative delirium. A detailed analysis is required to assess the specific risk of TKA in cognitive decline. Another limitation was that the number of patients in the delirium group was much smaller than that in the non-delirium group. There are also reports of subsyndromal delirium, which are not easily identified, but may be significant in terms of risks of falls and development of future dementia.[41, 42] Again, these may be identified by pre-operative cognitive function screening in a future study.
A prospective study in future with the accrual of more cases and routine delirium assessment may further our understanding of the risk factors for delirium.
{kind=link}
{kind=link}
{kind=link}