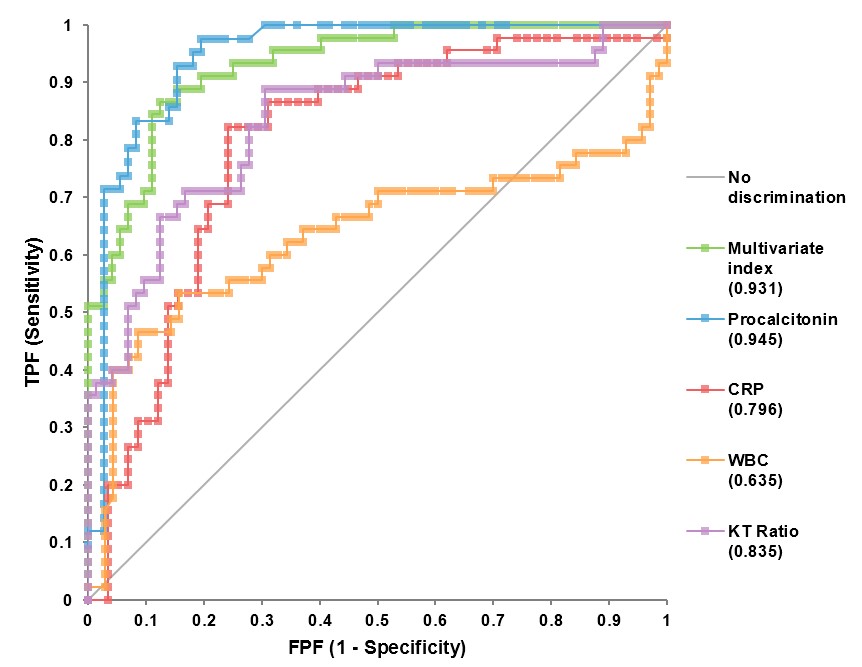
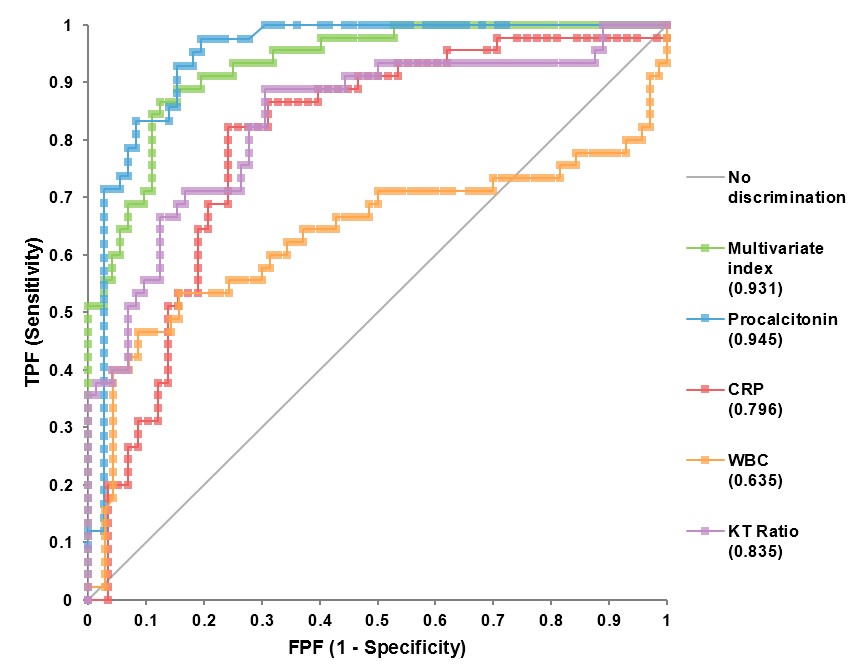
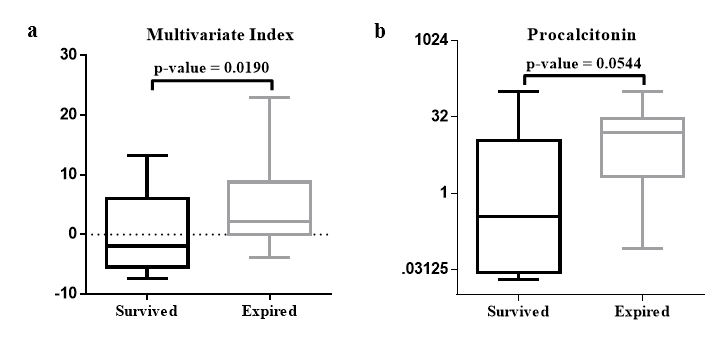
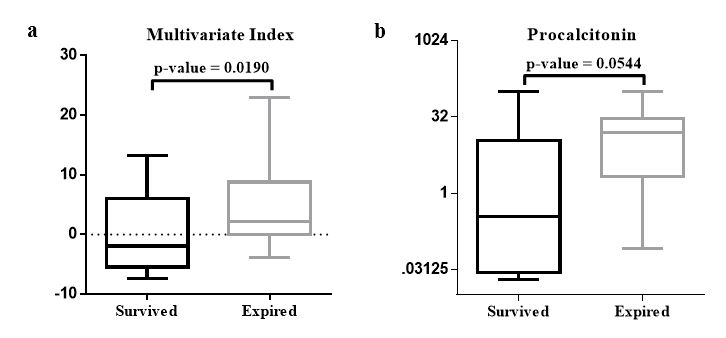
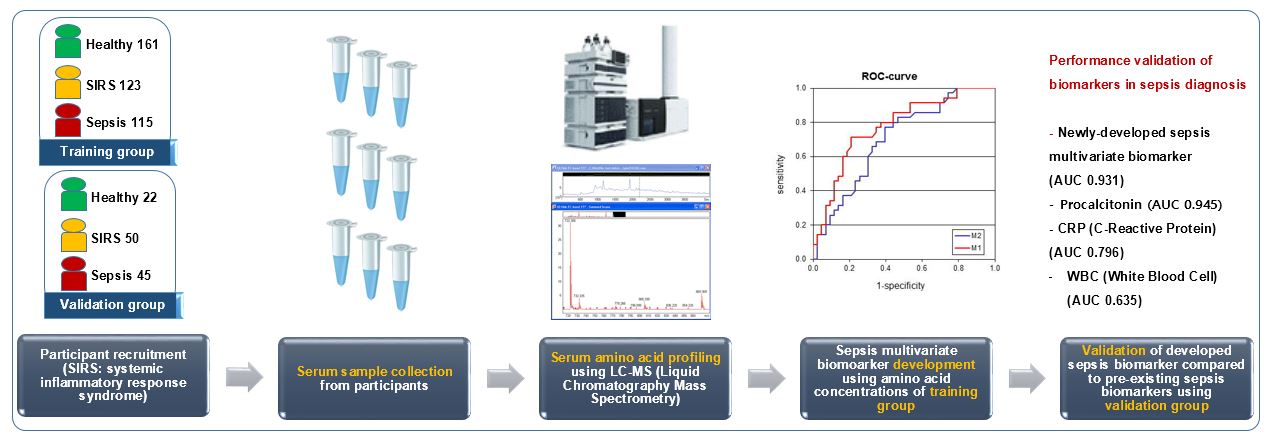
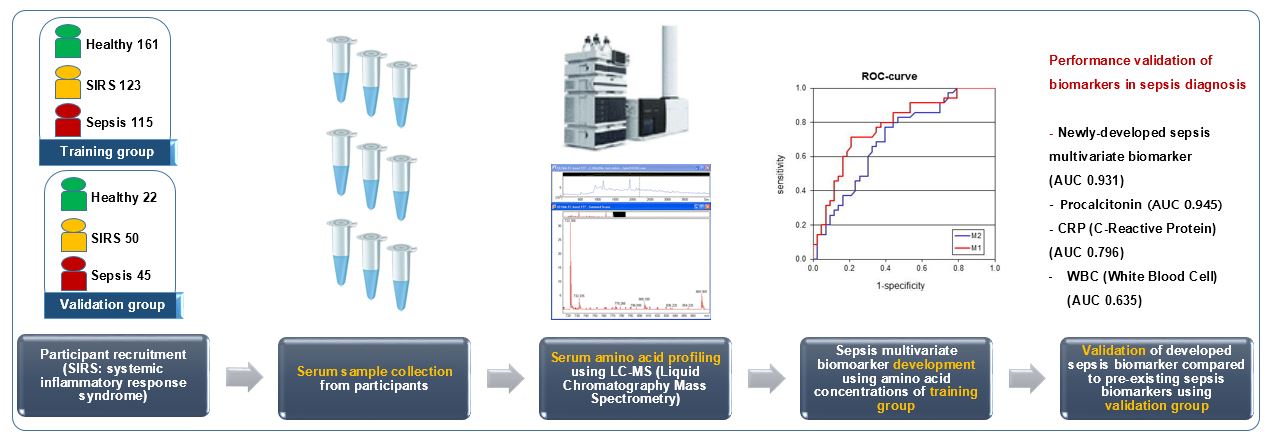
Herein, we found that amino acid metabolism in patients with sepsis is different from that in healthy individuals and patients with SIRS; indeed, the serum concentrations of some amino acids were significantly increased or decreased in patients with sepsis. We utilized these amino acids to develop a sepsis diagnostic biomarker in the form of multivariate index and validated its performance in the diagnosis of sepsis. The developed multivariate biomarker showed excellent performance in sepsis diagnosis with an AUC of 0.931 and exhibited a potential as sepsis prognostic biomarker.
In clinical practice, patients with sepsis typically exhibit significant heterogeneity regarding variables such as age, presence of underlying or secondary disease, state of the immune system, and infection severity. Moreover, the term “sepsis” covers a wide variety of pathophysiological processes that occur following infection [21]. Such features of heterogeneity increase the challenges of diagnosing sepsis timely and choosing the proper treatment methods for each patient. Therefore, a metabolomic approach would be preferred in treatment decision-making and prognosis of sepsis. Several researches have studied metabolomic derangements in sepsis [9, 22, 23]. Ferrario et al. [22] showed that low unsaturated long-chain phosphatidylcholine and lysophosphatidylcholine species were associated with long-term survival (90-day) together with circulating KYN in patients with septic shock. Rogers et al. [9] reported that due to metabolomic derangements, some metabolites, including KYN, were closely associated with 28-day mortality in critically ill patients. Furthermore, Cambiaghi et al. [12] reported that certain metabolites including KYN were associated with treatment responsiveness in the acute phase of septic shock. Although there are several previous studies on sepsis metabolism, this is the first attempt to develop sepsis diagnostic biomarker as a multivariate index using serum amino acid profiling.
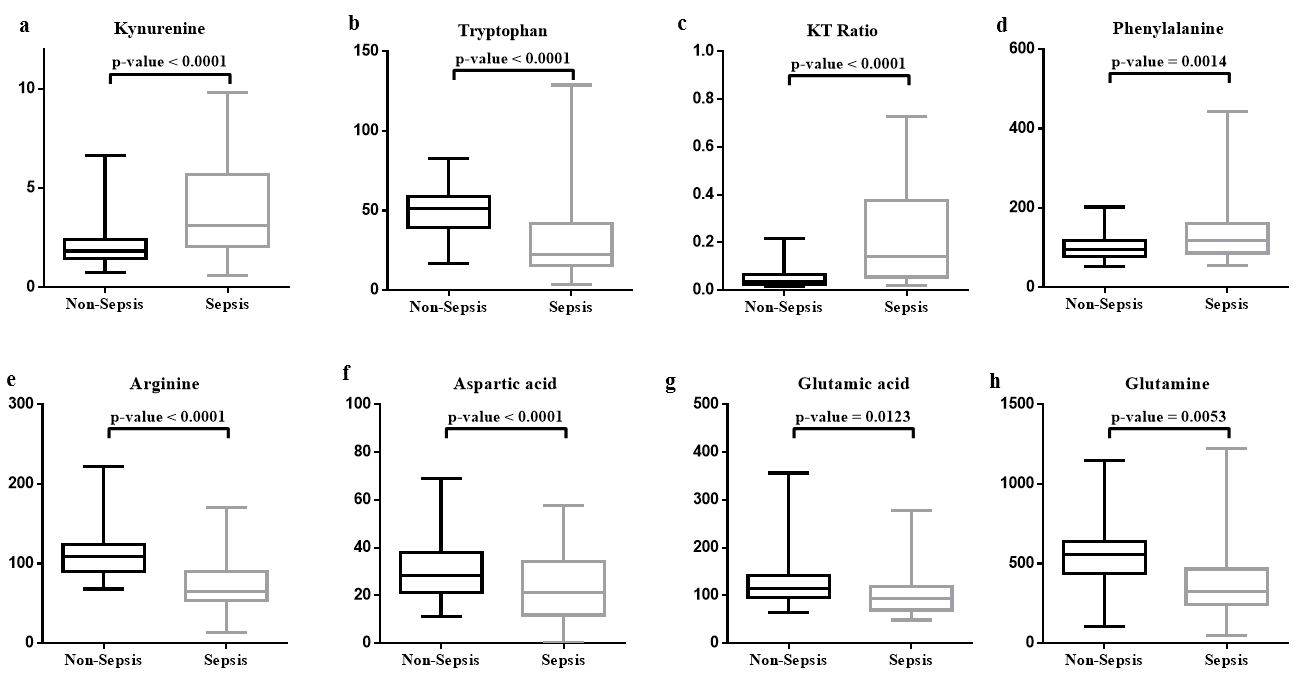
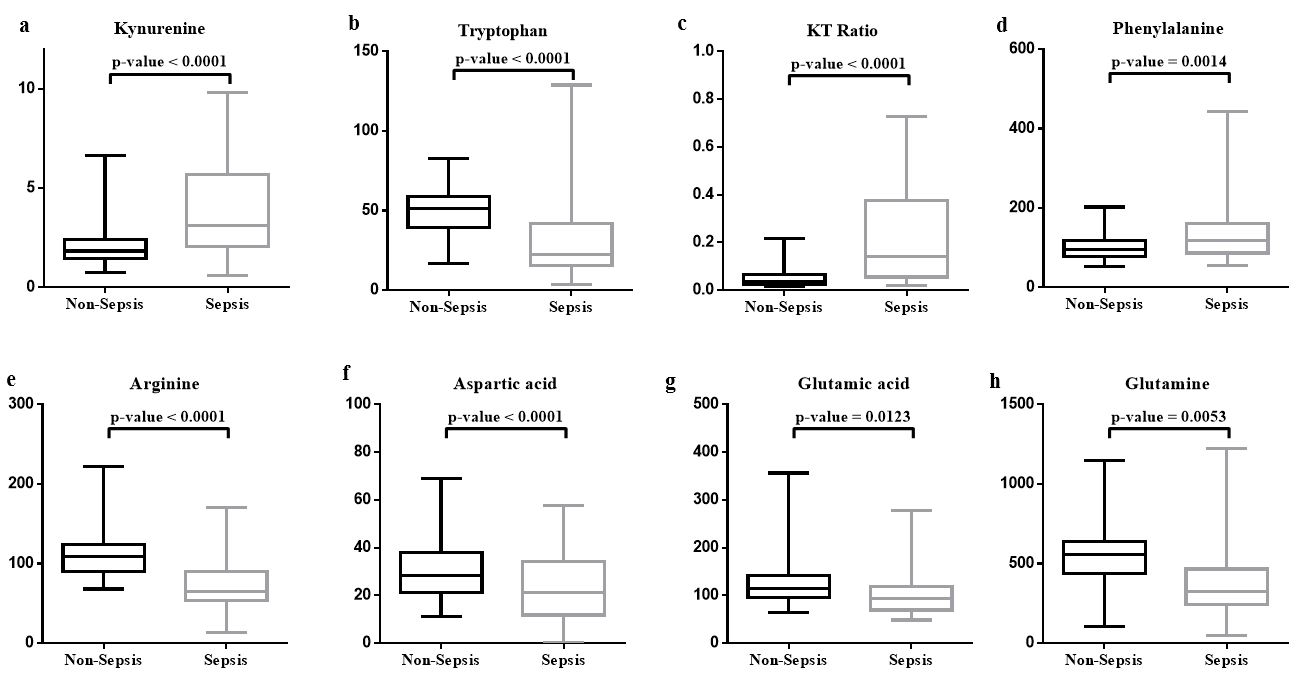
In the selection of candidate amino acids for developing the multivariate index, we considered the results of PLS-DA and comparison analysis of amino acid concentrations among subgroups, as well as data from the literature. Based on recent studies, all amino acids (TRP, ARG, and PHE) and the metabolite (KYN) included in the new multivariate index are closely associated with metabolic processes in patients with sepsis. The catabolic conversion of TRP to KYN occurs in sepsis by indoleamine-2,3-dioxygenase (IDO) [17, 19, 20, 24]. IDO is induced by interferon-gamma, toll-like receptors, and bacterial DNA, which are molecules related to infection and inflammation [18, 24, 25]. Therefore, KYN, TRP, and KT ratio are widely evaluated as indicators for sepsis, and recent findings have clearly revealed that increased KT ratio due to elevated IDO expression is a hallmark of bacterial infections such as in sepsis [25, 26]. ARG is an important initiator of immune response [27, 28]. Patients with sepsis present reduction in ARG synthesis in the kidney and increase in the synthesis of acute phase proteins, which contain ARG. Consequentially, ARG catabolism overrides anabolism in sepsis, and the serum levels of ARG decrease [29, 30]. PHE, which is a necessary precursor in the synthesis of catecholamines and thyroid hormone, is converted to TYR in the liver by phenylalanine hydroxylase (PAH), which is a sensitive hepatic enzyme [31]. Recently, a study revealed that increased PHE level in sepsis is indicative of insufficient conversion to TYR by PAH owing to damage caused to PAH cofactor, 5,6,7,8-tetrahydrobiopterin, by oxidative stress resulting from immune activation, such as sepsis [32]. Therefore, we could confirm that appropriate candidate amino acids, pathophysiologically related to sepsis, were selected to develop the multivariate index.
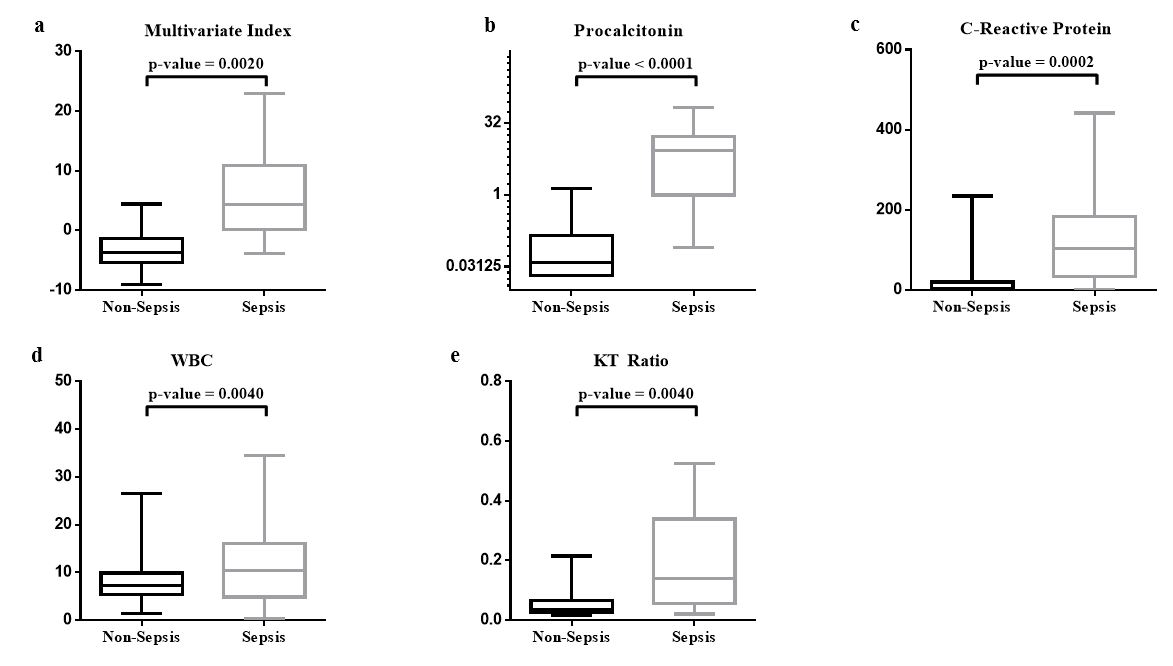
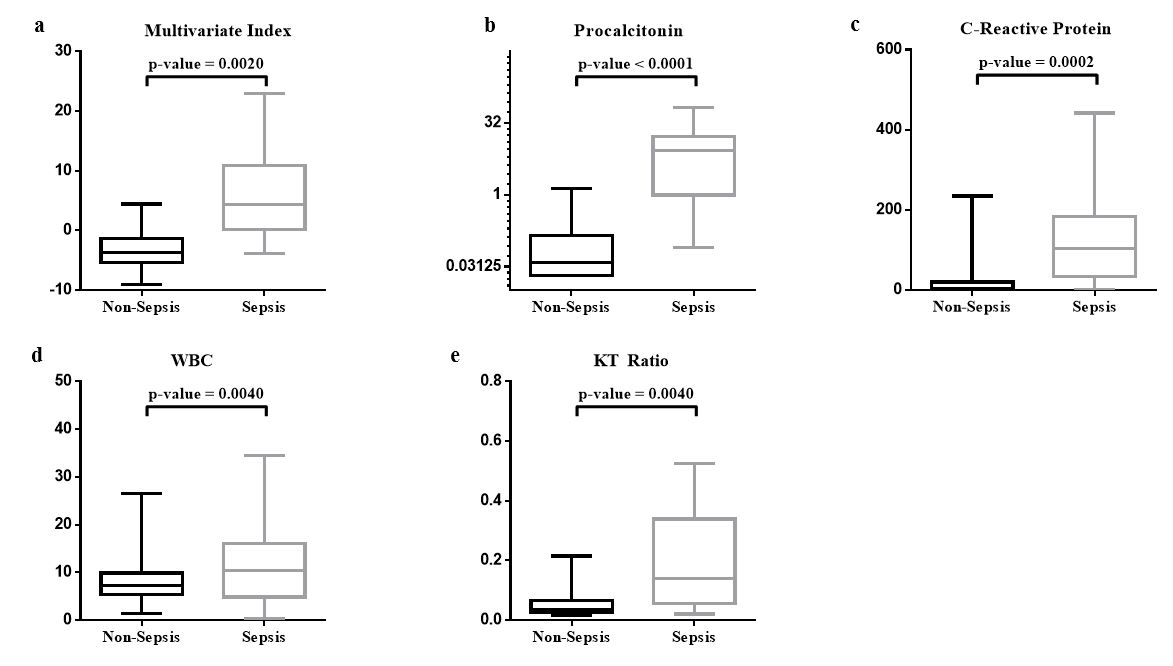
For the diagnostic performance of KT ratio, Zeden et al. [19] reported that the diagnostic AUC of KT ratio was 0.788 (95% CI, 0.644–0.912) in sepsis. However, in our study, the AUC of KT ratio alone was 0.835 and that of the multivariate index, which included PHE and ARG in addition to KT ratio, was 0.931 (95% CI, 0.887–0.974). Adding these two amino acids to the novel multivariate index showed better performance than that observed using KT ratio alone; however, further addition of amino acids such as ASP, GLU, and GLN did not improve the index clinical performance.
There are some limitations in our study. First, most of the pathogens infecting the patients with sepsis in this study were bacteria; there were few cases of fungal or viral infections. Since it is well known that serum PCT levels are significantly lower in patients with viral or fungal infections than in patients with bacterial infections [33, 34], these conditions could not be diagnosed appropriately using PCT. Moreover, patients with neutropenia were excluded from the study; however, PCT is produced by WBCs to some extent and, thus, the diagnostic performance of PCT in neutropenic status is expected to decrease [35]. In our study, the newly developed index and PCT showed the same excellent performance in sepsis diagnosis, and there was no significant difference between the two indicators. Therefore, to confirm whether the multivariate index has more strength in diagnosis of sepsis compared to PCT, a comparative study using patients with neutropenia or fungal infections is needed. Second, most of the patients with sepsis in the validation group had severe septic shock, which might have influenced the results of early sepsis biomarker evaluation. Septic shock is the most severe state of sepsis; therefore, more extensive biomarker changes may also appear. Previous studies using PCT have reported that PCT concentration was higher in septic shock than in sepsis cases, reflecting its severity [36, 37]. In our study, the AUC of both PCT and multivariate index was higher than 0.9 in the validation group. This value is relatively high when compared to those of other studies; Tang et al. [7] reported in their meta-analysis that the diagnostic performance of PCT, with an AUC of 0.78 (95% CI, 0.73–0.83), was not satisfactory for diagnosing sepsis. Tsalik et al. [37] also reported similar performance (AUC 0.78) of PCT predicting septicemia, which was relatively high compared to CRP and interleukin-6. Samraj et al. [38] reported better clinical performance of PCT with an AUC of 0.84 (95% CI, 0.75–0.9) for discriminating sepsis in children with cardiopulmonary bypass, but it was still lower than that in our study. Since most of the patients with sepsis in our validation group had severe shock, the diagnostic performance might have been overestimated compared to that in other studies. Therefore, further research is needed to confirm whether the multivariate index also shows a high diagnostic performance of an AUC of 0.9 or higher even at the early stage of sepsis unlike PCT. Finally, the novel multivariate index in our study is based on amino acid concentration measured by LC-MS/MS. However, LC-MS/MS is not widely distributed in front-line laboratories due to high cost, need of well-trained personnel, and low test throughput when compared to previously used automated chemistry analyzers. However, recently, matrix-assisted laser desorption ionization-time-of-flight mass spectrometer of small-size or for point-of-care testing has been introduced, and this type of point-of-care assay can be used instead of LC-MS/MS for amino acid concentration measurements with an easier operation method and short turnaround time, which improves the applicability of the test [39].
To our knowledge, this is the first study that utilized amino acid profiling for sepsis marker development using multivariate index. Moreover, we validated this multivariate marker for sepsis diagnosis in an independent patient group. It also included patients with SIRS, which is a condition barely distinguishable from sepsis when using pre-existing sepsis biomarkers. Furthermore, this study might improve the understanding of clinicians and researchers on the applicability of metabolomics in clinical medicine and the utility of multivariate index analysis as a tool for developing multivariate biomarkers showing good performance.
Concluding, we generated a simple and of high-performance multivariate sepsis biomarker, highly specific for sepsis diagnosis using only four serum amino acid concentrations. Moreover, it showed potential as sepsis prognostic biomarker. Our study demonstrated that serum amino acid profiling in the diagnosis of sepsis could yield promising results because it depicts the individual characteristic metabolic state, which would enable and help clinicians to use tailored medicine, ensure early diagnosis and timely adequate treatment, and precisely predict prognosis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}