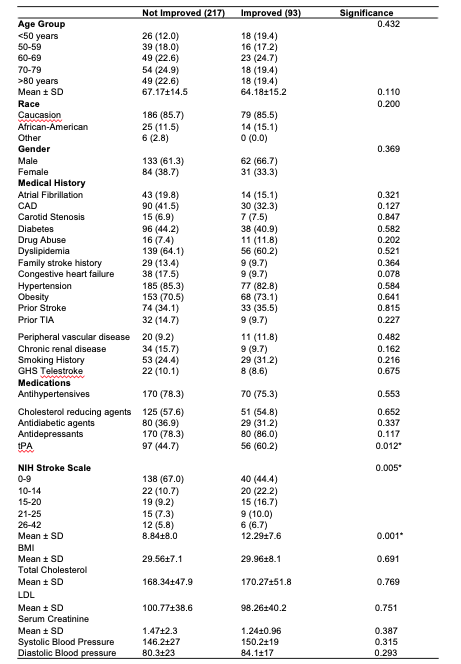
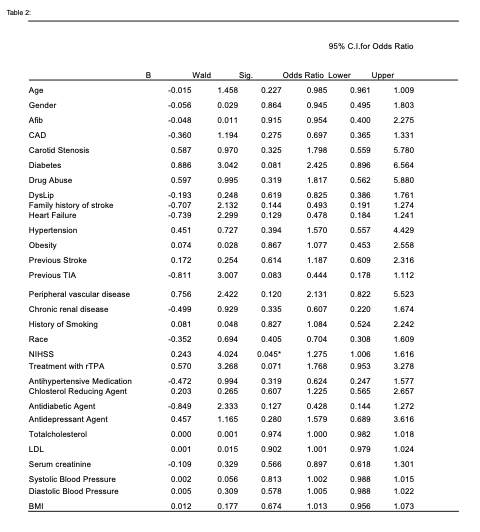
The goal of this study was to investigate clinical risk factors that may be associated with an improvement or no improvement in the recovery of ambulatory functions following thrombolysis therapy in acute ischemic stroke patients with pre-stroke depression. In the univariate analysis, we found that the proportion of ischemic stroke patients with pre-stroke depression who presented with no improvement in ambulation after treatment with rtPA was higher than those with an improvement in ambulation. This may be linked to differences in the proportion of clinical factors between patients that presented with an improvement and those with no improvement in their ambulation status. We expected that the use of antidepressants would be identified as a variable associated with ambulatory status. However, the univariate analysis as well as the adjusted analysis did not reveal a significant association of antidepressants with ambulatory outcome in ischemic stroke patients with pre-stroke depression treated with thrombolysis therapy. It is possible that the variation in the effects or use of antidepressants may be associated with stroke severity, rather than with the ambulation status.
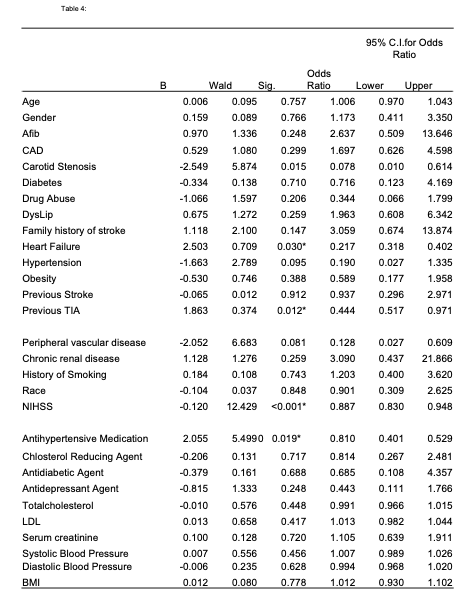
In the univariate analysis, NIHSS (indicator of stroke severity) was associated with a significant improvement in ambulation among ischemic stroke patients with pre-stroke depression. This effect was sustained in the adjusted analysis for the total population of ischemic stroke patients with pre-stroke depression and was associated with no improvement in the group with no improvement in ambulation following rtPA. In general, the initial NIHSS score is a strong predictor of stroke severity and may predict functional outcome as well. In the univariate analysis, stroke severity, demonstrated by NIHSS, was between 0 and 14 for many of the patients with no improvement following treatment with rtPA. The adjusted analysis associated initial NIHSS with both an improvement and no improvement in ambulation following rtPA. This finding indicates that the severity of stroke is not enough to predict functional ambulatory outcomes, and that clinical risk factors may as well play a significant role [26, 27].
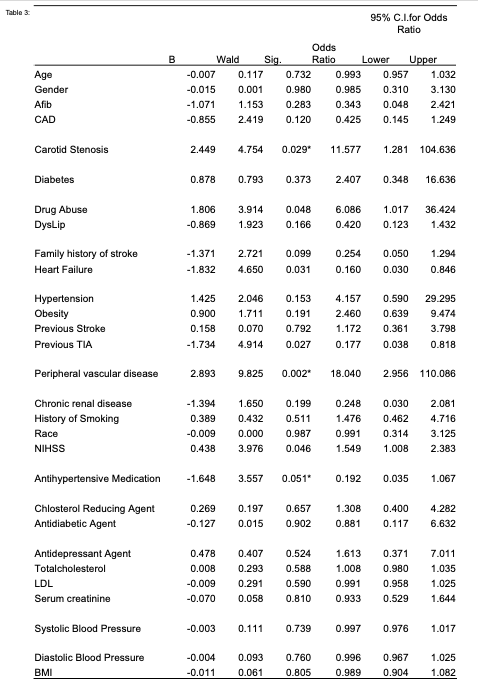
In the population that presented with an improvement in ambulation, we observed that in the adjusted analysis, patients that presented with carotid artery stenosis and peripheral vascular disease were more likely to be associated with an improvement in ambulation. However, patients that took antihypertensive medications were more likely to be associated with no improvement following thrombolysis therapy. Because clinical risk factors associated with an improvement in functional ambulatory recovery maybe be different between the population with an improvement and those with no improvement, we performed additional analyses to evaluate if these factors may significantly differ. Our findings indicate that in the no improvement group, the effect of carotid artery disease and peripheral vascular disease, which were significant in the improvement group, were attenuated in the no improvement group. Moreover, our adjusted analysis revealed that previous TIA, congestive heart disease, and use of antihypertensive medications were more likely to be significantly associated with no improvement in functional ambulatory recovery in ischemic stroke patients with pre-stroke depression.
Previous TIA is not a formal contraindication for rtPA, especially if the TIA was at least three months before the onset of stroke [28] [22, 29]. However, it has been shown that the onset of TIA within 24 hours of stroke may lead to a poor outcome following rtPA [30, 31]. It is possible that some ischemic stroke patients with pre-stroke depression may present an invisible TIA in the CT scans making it difficult to detect. and this may affect treatment outcome with rtPA. This might be the case in ischemic stroke patients with pre-stroke depression that received rtPA resulting in no improvement outcome in functional ambulatory recovery. The association between antihypertensive medication and depression is well documented in the literature[32, 33]. It is known that if depression occurs prior to stroke, medication use plays a role in the treatment outcome of the stroke[21, 34]. It is also known that clinical risk factors contribute to, or worsen, the underlying disease such as depression and stroke [28]. However, the relationship between certain clinical risk factors, such as congestive heart failure, with treatment response to rtPA and functional ambulatory outcome in ischemic stroke patients with pre-stroke depression is not known.
Depression is an independent risk factor for the onset of congestive heart failure [35, 36], and subclinical depressive symptoms are also correlated with an increased risk of stroke[37]. The biological variables that trigger this relationship are due to multiple alterations in neuroimmunoendocrine proteins in depressed patients, especially in the acute phase[38]. It is not clear how these factors interact with rtPA to affect functional ambulatory recovery in ischemic stroke patients with pre-stroke depression, and this is beyond the scope of the current study. However, ample evidence indicates that congestive heart failure may have a causal relationship with depression in stroke patients[39-42]. This is especially important since certain areas in the brain, including the medial temporal region, an area associated with the pathophysiology of depression, are particularly vulnerable to perfusion deficits which arise in the context of congestive heart failure[43, 44]. Clinically, our results indicate that congestive heart failure, antihypertensive medications, and previous TIA are important clinical risk factors that may affect the treatment outcomes of thrombolysis therapy and affect functional ambulatory recovery in ischemic stroke patients with pre-stroke depression. Our findings have practical implications and suggest the need for the development of an effective strategy to manage the combined effect of congestive heart failure, antihypertensive medications, and TIA in ischemic stroke patients with pre-stroke depression.
Our study has limitations. The retrospective nature of our data may indicate the possibility of selection bias. In addition, the absence of pre-stroke functional status data including pre-stroke mRS and post treatment NIHSS scores did not allow for the comparison of ambulatory recovery and NIHSS scores or mRS to be evaluated. Depression is a common post-stroke complication and pre-stroke depression is known to contribute to treatment outcome following thrombolysis therapy. An important contribution of the current study to existing literature is identification of specific clinical risk factors that are significantly associated with functional ambulatory outcome in ischemic stroke patient with incidence of pre-stroke depression who received thrombolysis therapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}