In current prospective cohort study, we indeed reveal that patients with DKD exhibited higher renal fibrosis (corresponding to lower D value) and worse hypoxia (corresponding to higher R2* value) compared to non-DKD, and the index of fibrosis (CD values) and hypoxia (MR2*) deteriorated by the decline of renal function. Further, either increased MR2* or decreased CD strongly correlated with poor outcomes of patients with DKD. Importantly, integrating MR2* and CD markedly increased the efficiency in assessment of DKD prognosis compared to each single of them respectively.
Accumulating evidence have emphasized the roles of renal tissue hypoxia and fibrosis [25, 26] in the progression of CKD regardless of etiology[27]. Although oxygen-sensitive microelectrodes could directly measure tissue oxygenation and the degree of fibrosis could be evaluated by biopsy, the highly invasive damage is the main obstacle in clinical practice [28]. Functional MRI is able to identify the signals of hypoxia and fibrosis in kidney simultaneously by the measurable translating values derived from fMRI images [29].
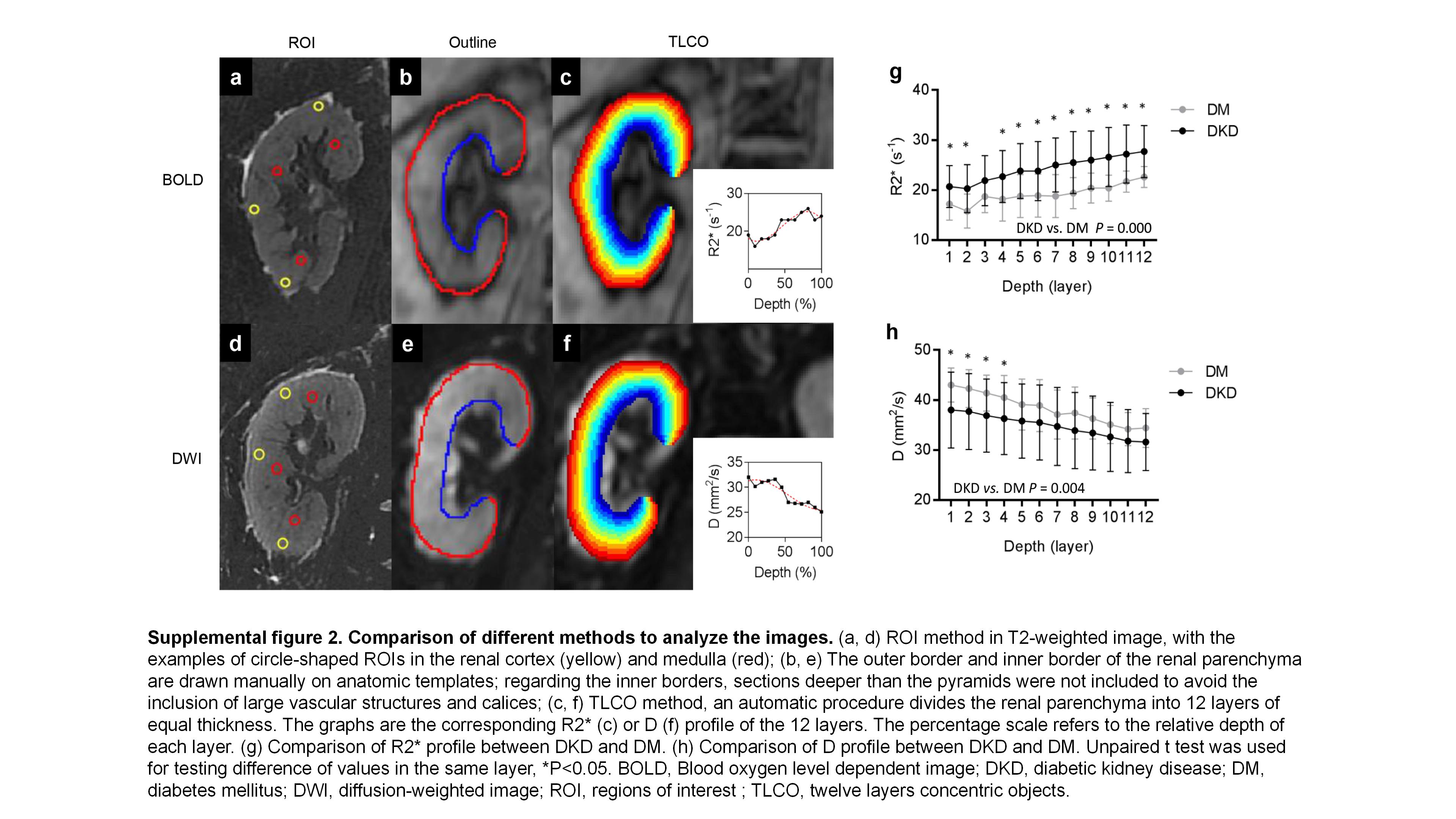
Our data demonstrated that the profile of R2* in DKD markedly increased compared to non-DKD, especially in advanced stages, which supported that renal hypoxia increased with progression in DKD (Fig. 1e and 1f). Higher R2* heralded a worse outcome (AUC was 0.80, as shown in Fig. 3b). Of note, part of patients were placed on long-term treatment of loop diuretics, for example, furosemide which inhibits sodium reabsorption, consequently, may decrease oxygen consumption[30, 31], because loop diuretics block the Na+-K+-2Cl− transporter in the thick ascending loop of Henle, and increase local pO2 [32]. Besides, factors that affect the oxygen dissociation curve influence the BOLD-signal, such as body temperature, blood pH etc., make it inexact to predict prognosis with R2* value alone [33–36]. Thus, alternated method of fMRI called IVIM was applied in clinical practice recently.
The D value derived from IVIM reflects pure molecular diffusion, because it minimizes the influence of blood flow on tissue diffusion. The aggravation of DKD architectural malformation and the increased cell density destroy the microcirculation and affect the diffusion of water which restricts water molecule movement in turn exhibits a lower D value [37, 38]. Several studies have shown that IVIM is sensitive to renal dysfunction, renal artery stenosis, allograft rejection, and the early changes in DKD [39]. Although the D value decreased with renal dysfunction and predicted a poor outcome in current study (AUC = 0.77), we supposed that the combination of R2* and D may improve the efficiency of prediction. Our results demonstrated both MR2* and CD strongly correlated with the outcomes of DKD. It is noteworthy that the combination of MR2* and CD was more significant than each single value (Fig. 3f) to predict the prognosis.
The potential pernicious influence of etiology diversity on the MRI detectable values in kidney was decreased, for all the patients were confined in a scope of DM patients; and consequently, the homogeneity of disease made the comparison valid. We found that the correlation of poor outcomes of DKD with basic fMRI values was confined not only in the cortex but also the medulla. Previous studies reported that oxygenation in cortex other in medulla decreased in CKD [11, 24], because the reduction of blood flow in cortex [25] impacted on eGFR decline more than that in medulla [11]. However, renal medulla was relative hypoxic and more vulnerable to hypoxia compared to cortex as found in our results.
In our study, all patients were screened within average age of about 50-year-old and 10-year DM-duration, which were matched to non-DKD controls. To diminish the impact of long time observation for DKD, 35 of 77 patients at stage of CKD 3–4 were chosen; it enables us to observe the end point in relative short time. The age-, DM duration- and gender matched controls made the data comparable. Although a study displayed the positive relationship between R2* values and age [40, 41], our age- and gender- adjusted multivariable analysis (Table 1) proved R2* and D values were significantly associated with outcomes of DKD. We did not reveal that the correlations of age, ACR and the DM duration with the clinical outcomes of DKD, the underlying reasons might be the strict inclusive criteria and relative short follow-up time.
The perspective strengths of present study are the prospective cohort design, strict inclusive criteria, and the use of a well-validated protocol including reproducible analysis method of fMRI. To reduce the influence of hydration status on the BOLD signal [42], all the participants were asked to stop taking diuretics a day in advance, fasting and water-deprivation were conducted 6 hours before the examination. To avoid a system bias, we applied a validated TLCO technique, which integrates geometrical information and takes into account the entire renal parenchyma. The intervening measure mentioned above made it more sensitive to identify the differences than the partial harvested data and shows excellent reproducibility and lower variability.
A limitation of current study is that a relative high percentage of advanced DKD enrolled. It shortens the time for observation, but the complications coming up with advanced DKD decreased the validation of current conclusions. Then, we did not have the histologic “gold standard” for all the participants to validate MRI data, although renal biopsy was also limited in predicting the decline of renal function in DKD. Last, we did not monitor the level of hypoxia and fibrosis by a second- or a third-time MRI, which would enable us to evaluate whether the long-term changes in kidney were consistent with the development of DKD.
In summary, this study describes the prediction value of fMRI in the assessment of DKD prognosis. Although fMRI is so far largely restricted in the research setting, our study indeed demonstrates that the values derived from fMRI correspond to hypoxemia and fibrosis in kidney, consequently, project the outcomes of DKD.
{kind=link}
{kind=link}