We have presented the 20-year experience of a tertiary referral center in the surgical management of midfacial tumors. Neoplasias of the midface have a variety of tumor cells biological aggressiveness and their different response to the surgical treatment create the need of a management plan tailored to every patient. Since the beginning of the century, Sigmund Freud and the President of the USA were the first patients treated for maxillary tumor [12]. Squamous cell carcinomas represent more than 90% of all malignant neoplasms of the oral cavity and have a high correlation with alcohol consumption and smoking [13]. The surgical resection of midfacial tumors along with the subsequent reconstruction is a demanding and challenging procedure that must be carried out by specialized surgeons.
As midfacial neoplasias tend to be asymptomatic until late stages, the primary tumor has often spread into adjacent structures and anatomical spaces; The Ohngren’s classification, a prognostic examination, is an imaginary plane extending b/n medial canthus of eye and angle of mandible. Supra structural growth situates above this plane have poor prognosis and infra structural growth below this plane have better prognosis; It is vital to use every available diagnostic examination to depict the spread of the tumor and make the appropriate surgical plan [14] in more details. Biopsy results are essential for the clarification of the type of the tumor, which will determine the surgical approach. Flexible endoscopy can be used to assess or biopsied the lesions from nasal or naso-pharyngeal tumors. Standard x-rays can show bone destruction and opacification of sinuses. CT scans may help the assessment of soft tissues, bony involvement, local spread and node status. MRI scans may differentiate inflammation, oedema, and mucous from tumor and peri-neural spread, as well as ruling out intracranial extension. Deeply located tumors may be accessed by a CT-guided needle biopsy. Angiography has a limited role and it is mainly addressed to vascular tumors, such as juvenile angiofibroma, for the identification and embolization of feeding vessels [15].
Maxillectomy is used to remove damaged parts pf the maxilla due to cancerous tissues. The first maxillectomy was performed in the late 1820s, and since then a significant evolution of midface surgical approaches has been observed. Based on the Algorithm of Corderio, removal of midfacial neoplasias may be classified as partial, subtotal, total, or radical maxillectomy [16]. In partial maxillectomy, part of maxilla is removed leaving one or more bony walls in place. It often includes alveolectomy or medial maxillectomy. Subtotal maxillectomy is defined as a partial maxillectomy with total palatectomy. Total maxillectomy involves removal of the whole maxilla. Extended or radical maxillectomy, described in 1954, includes a total maxillectomy and palatectomy defect with loss of orbital support or eye. When maxilla is removed, a prosthesis obturator is used to seal the opening between mouth and nose, in order to prevent fluid and food ascending to the nose, to improve speech postoperatively and to provide a better aesthetic image. In addition, tumor involving the orbital periosteum is an indication of orbital exenteration. Maxillectomy in combination with orbital exenteration or orbitectomy and anterior fossa resection were mostly used in our case series [17, 18].
Excision of midfacial tumors can be performed through four main surgical approaches. Intraoral approaches include direct excision, facial degloving, and LeFort 1 maxillotomy. Subtotal maxillectomy via transfacial approach be used for early diagnosed and well localized intraoral tumors. Facial degloving approach, popularized in 1970, provides access to both maxilla and the nasal cavity, allowing complete bilateral exposure of the midfacial skeleton, without any visible incisions [19]. Zachariah et al reported excellent outcome with this approach in 9 patients [20]. LeFort 1 maxillotomy is used to approach nasopharyngeal tumors through osteotomy of the maxilla, without facial incisions [21–23]. Transfacial approaches include the modified Fergusson approach which, through a lateral rhinotomy incision extending infraorbitally, may expose the whole maxilla [24] while the maxillary swing provides access to the nasopharynx and the skull base [25, 26]. The temporal approach, first mentioned in 1985, provides access to the posterior maxilla, the retromaxillary region region, and the orbits, without disturbing functional anatomy nor facial incisions [27, 28]. The craniofacial approach provides access to intracranial portions of midfacial tumors, with stroke, epilepsy and intracranial infections as reported complications [28].
Postoperative facial disfigurement affects social life significantly [8]. However, patients treated with midfacial implant-retained prostheses state that the prosthesis removes their fear of unwanted attention and increases their overall quality of life [10, 29]. Subjective health-related quality of life was found reduced in comparison with preoperative facies when the acquired defects were located in the region of the eye and the nose [30].
The order of reconstruction in midfacial tumors depends on the size of the defect [31, 32]. Maxillary defects are characterized by the extent of resection of critical midfacial components. Reconstruction of the infraorbital rim and orbital floor optimises appearance and function [1]. There are many available reconstruction options based on Algorithm of Corderio [6]: Prosthetic obturation, autogenous flaps (pedicled flaps, vascularized free flaps, non-vascularized autogenous bone grafts or combinations), allografts and alloplastic materials (titanium mesh, dental implants). The advantages of the obturators in functional rehabilitation should not be overlooked. The use of obturators shortens the duration of surgery and hospitalization, provides better visualization for follow-up, facilitates speech and swallowing and restores cosmetic appearance. They are placed intraoperatively and they are removed in 2 weeks. Then an interim obturator may be used until final healing, when a definitive obturator is placed about 6-12 months postoperatively [17, 18].
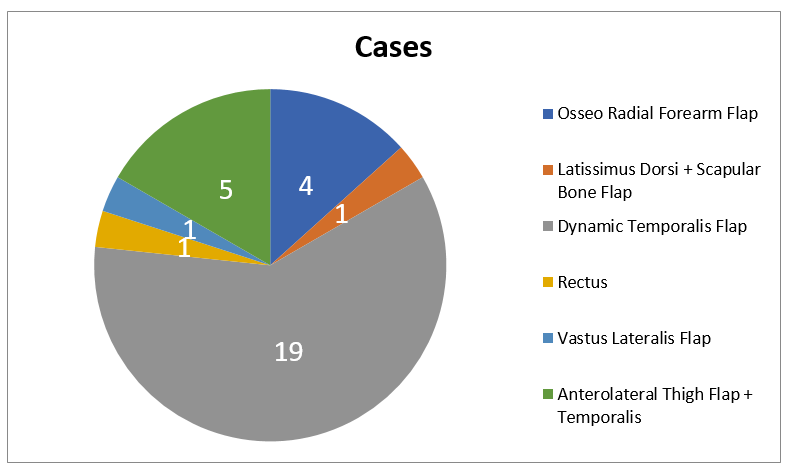
Many pedicled flaps, local or regional, have been used for midface and maxillary reconstruction. They can be easily harvested; however, they are limited by their feeding vessels. Local flaps include buccal fat pad flaps, palatal island flaps, nasolabial flaps, tongue flaps and uvula flaps. Regional flaps include submental flaps, temoproparietal-galea flaps, temporalis flaps, platysma flaps, masseter flaps, sternocleidomastoid flaps, trapezius flaps, deltopectoral flaps and pectoralis major myocutaneous flaps, successfully used to cover midface and maxillary defects [33]. We have used lengtheming temporalis myoplasty flaps in 18 patients in our study, as it an easy flap with reliable blood supply and abhidden incision.
Evolution of surgical techniques with the applications of free flaps has broadened the horizons of reconstruction radical surgery, as they can be successfully used to cover large tissue defects after radical midface surgeries. Parts of the skull base may be removed and the risk of meningitis is minimized when the cavities are sealed with vascularised tissues [34, 35]. Vascularized free flaps include radial forearm free flaps, radial forearm osteo-fascio-cutaneous flaps, rectus abdominis flaps, fibula osteo-cutaneous flaps, scapular osteo-myocutaneous flaps and vascularized iliac crests [36–38]. We have chosen to use radial forearm osteo-fascio-cutaneous flaps in 4 cases, as it is useful for smaller reconstructions, it can be easily harvested and often provides good skin color match for head and neck reconstruction. Moreover, Yetzer J et al presents its usefulness in palatal defects [39]. In one case, we have used a rectus abdominis flap providing an appropriate tissue bulk with a pliability while it may cause abdominal weakness and hernia formation [36]. Moreover, in 5 cases with posterior palatomaxillectomy defects, we have used an anterolateral thigh flap, which provides significant tissue bulk and a long pedicle, allowing the primary closure of the donor site [14, 36].
Complications during treatment stages are not uncommon and patients should be informed about the possibility of the necessitation of multiple surgical procedures before the final outcome [14]14. Total failure of the flap is a rare but severe complication, often caused by thrombosis of the flap vessels and demands intensive flap checks, especially in the first 3 postoperative days [40]. Costa et al reported 4% loss of flap in 24 years [41]. No such complication was observed in our study.
Our study has a limitation. This is a retrospective case series, with no comparison group. We believe that the experience of a tertiary referral center, such as ours, is valuable for the formulation of management protocols and the provision of guidelines for the appropriate choice of surgical management.
In conclusion, tumors of the midface encompass a diverse group of neoplasias. Surgery is the gold standard of treatment and its goals are complete oncological resection of the tumor and surgical reconstruction is essential in restoring quality of life and social functioning of patients with extensive midfacial defects. Optimal management of patients with midfacial defects should involve a multidisciplinary approach and the patients should be informed about all surgical options and likely outcomes. The results of our study have confirmed that surgical treatment may have satisfactory results when performed by experienced and specialized surgeons in tertiary centers. Midface resection can be safely performed with a combination of microvascular and dynamic reconstruction of the face offering our patients a better quality of life.
{kind=link}