Characteristics of respondents
Four hundred thirty-six study participants were involved in the analysis with response rate of 98.9%. The mean age of the study participants was 37.87 with standard deviation (SD) of 12.5 with females constitute 192 (44%). More than half (58.5%) were protestant followed by orthodox and Muslim constituting 25% and 15.4 % respectively. More than three fourth (83.5%) were married. Hundred seventy-seven (40.6%) of them achieved college and above level. Nearly one quarter (32.6%) of the total study participants were government and/or nongovernmental organizations’ employees and 157 (36.0%) of them rely on their salary to live.
Community risk assessment and awareness
There are at high risk individual in 115 (26.4%) of the visited households (either age or underline medical condition). One hundred seventy-nine (41.1%) of the participants perceived they have high risk of contracting COVID-19. Four hundred two (92.2%) of the respondent knows how to protect oneself from COVID-19. Four hundred twenty (96.3%) of the respondent reported they get information about COVID-19 from TV/radio (Table 1).
Table 1: Community risk and awareness assessment among dwellers of selected towns, west Oromia, Ethiopia, Aug, 2020, (n=436)
|
Variables and description
|
Number
|
%
|
|
Household (HH) members traveling from place to place
|
Yes
|
109
|
25
|
|
No
|
327
|
75
|
|
Presence of health care worker in the HH
|
Yes
|
40
|
9.2
|
|
No
|
396
|
90.8
|
|
Presence of highly mobile individual in the HH
|
Yes
|
135
|
31
|
|
No
|
301
|
69
|
|
High-risk individuals in the HHs
|
Yes
|
115
|
26.4
|
|
No
|
321
|
73.6
|
|
Perceived level of risk for contracting COVID-19
|
High
|
179
|
41.1
|
|
Medium
|
107
|
24.5
|
|
Low
|
134
|
31.7
|
|
Do not Know
|
16
|
3.7
|
|
Visited by health extension workers (HEWs)
|
Yes
|
127
|
29.1
|
|
No
|
309
|
70.9
|
|
Frequency of visit by HEW
|
Once
|
77
|
60.6
|
|
Twice
|
38
|
29.9
|
|
Three or more times
|
12
|
9.4
|
|
Ever heard about COVID-19
|
Yes
|
428
|
98.2
|
|
No
|
8
|
1.8
|
|
Source of information about COVID-19
|
Television /radio
|
420
|
96.3
|
|
Social medias
|
271
|
62.2
|
|
Health professionals
|
208
|
47.7
|
|
Religious leaders
|
141
|
32.3
|
|
Community leaders
|
129
|
29.6
|
|
Family members
|
98
|
22.5
|
|
What the participants know about COVID-19;
|
don’t know anything
|
38
|
8.7
|
|
It’s a virus that can cause a disease
|
389
|
89.2
|
|
It’s a government’s program
|
2
|
0.5
|
|
It’s a TV/radio campaign
|
2
|
0.5
|
|
Other*
|
5
|
1.1
|
|
Kind of information gained
|
Protection methods
|
402
|
92.2
|
|
Symptoms
|
384
|
88.1
|
|
Transmission ways
|
366
|
83.9
|
|
Actions taken when contract COVID-19
|
258
|
59.2
|
|
How dangerous COVID-19 is;
|
Very dangerous
|
353
|
81
|
|
More or less dangerous
|
72
|
16.5
|
|
Is not dangerous
|
7
|
1.5
|
|
Other**
|
4
|
0.9
|
|
Possibility to be infected by COVID-19
|
Yes
|
287
|
65.8
|
|
No
|
122
|
28
|
|
Don´t know
|
27
|
6.2
|
Key: Other * (it is curse of God, is intentional product from other countries), other** (it is fatal, it comes and go)
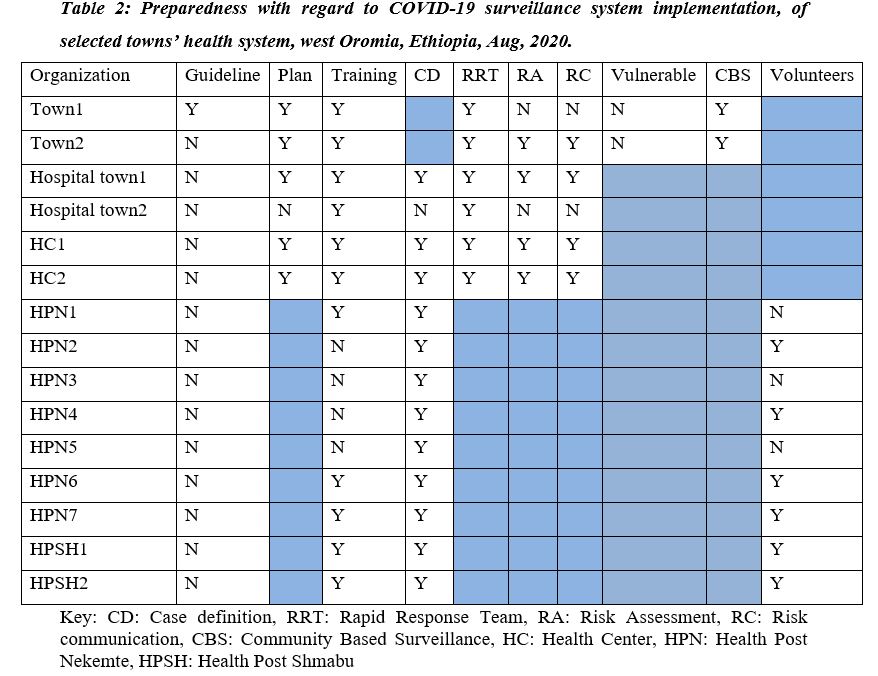
Health system Preparedness
Two hospitals, three health centers, one town health office, one zonal health department and nine health posts were participated in the study. Only 1of 15 (6.7%) organization assessed have guideline/manual of COVID-19 surveillance. All health centers, hospitals and health offices were trained on COVID-19 surveillance system while 4 (44%) of the interviewed health extension workers reported they didn’t get training. Three (33%) of the assessed health posts didn’t have community volunteers. Rapid Response Team (RRT) has been established at all levels in the towns. Updated case definition is found in 14/15 (93.3%) of the visited facilities.
In both towns, preparedness with regard to implementing surveillance system from plan to community engagement is presented as follows (Table 2).
Surveillance performance
Suspect identification and reporting
Community experience and practices
Four hundred twenty-five (97.5%) of the participants reported that they will report to health system, either to local health unit or call 8335, if they suspect individual with COVID-19. From the total visited households, 182 (41.7%) reported that their health care visiting experience have been affected by the emergence of COVID-19. One hundred ninety-seven (45.2%) reported that they are not using health facilities for routine services during this pandemic. Among those who reported not using health facility during this pandemic, 132 (66.7%) were not using health facilities because they fear of contracting COVID-19 (Figure 1). Majority, 409 (93.8%) of the respondents reported that they are willing to be isolated if get infected (Table 3).
Table 3: Community experience and practices assessment towards COVID-19 in selected towns, west Oromia, Ethiopia, Aug, 2020, (n=436)
|
Variables
|
Description
|
Number
|
%
|
|
Experience during feeling ill health
|
Visit health facility
|
360
|
82.6
|
|
Go to pray
|
47
|
10.8
|
|
Purchase some medicine
|
23
|
5.3
|
|
Eat foods believed to be remedy
|
4
|
.9
|
|
Othersa
|
2
|
.5
|
|
Access to health services affected
|
Yes
|
182
|
41.7
|
|
No
|
254
|
58.3
|
|
Using health facilities during the pandemic
|
Yes
|
239
|
54.8
|
|
No
|
197
|
45.2
|
|
Willing to be isolated if contract COVID-19
|
Yes
|
409
|
93.8
|
|
No
|
27
|
6.2
|
|
Practices if contract COVID-19
|
I will take locally advised foods, garlic, ginger, soups etc..
|
227
|
52.1
|
|
I will go to the hospital / health unit
|
400
|
91.7
|
|
I will go to the neighborhood nurse
|
46
|
10.7
|
|
I will buy medicines at the market
|
19
|
4.4
|
|
I will look for the traditional healer
|
12
|
2.8
|
|
I would stay in quarantine
|
161
|
36.9
|
|
Action to be taken on suspecting person with COVID-19 symptoms
|
Report to local health
|
256
|
58.7
|
|
Call 8335 or local call center
|
169
|
38.8
|
|
Do nothing
|
1
|
0.2
|
|
do not know
|
10
|
2.3
|
|
heard someone died of COVID-19
|
Yes
|
13
|
3.0
|
|
No
|
423
|
97.0
|
|
Heard neighbor died of COVID-19
|
Yes
|
9
|
2.1
|
|
No
|
427
|
97.9
|
others include: do nothing, stay at home
Health system performance
House to house visit for risk group identification and suspect identification was done only between April to May, 2020. Between these periods, 12,012 of 25,413 (47.2%) households in Nekemte town have been visited by health extension workers to identify 7 suspects of which 3 became positive for COVID-19. In Shambu town, 3,012 of 3,931 (76.9%) households have been visited, but no data was available that indicate the number of suspects identified and tested.
At facility level, there was no screening service at triage in both towns. Individual will be suspected for COVID-19 when assessment is conducted at outpatient department. Up to now, 173 suspects have been identified from Nekemte town, none of which were positive. Whereas, 144 suspects have been identified from Shambu town of which 4 were positive. No rumor and cluster investigation practiced at both towns (Table 4).
Table 4: Suspect identification and testing by health system level, COVID-19 surveillance system evaluation, Western Oromia, Ethiopia, Aug, 2020.
|
Level
|
Town
|
Suspect identified
|
Suspect Tested
|
Result
|
|
Positive
|
Negative
|
Pending
|
Blank
|
|
Health post
|
2
|
7
|
7
|
3
|
4
|
0
|
0
|
|
1
|
Data not available
|
|
Health facility
|
2
|
124
|
124
|
0
|
121
|
3
|
0
|
|
1
|
144
|
144
|
4
|
140
|
0
|
0
|
|
RHB (suspect investigation data)
|
2
|
35
|
35
|
1
|
29
|
5
|
0
|
|
1
|
1
|
1
|
1
|
0
|
0
|
0
|
|
RHB (laboratory-based surveillance data)
|
2
|
115
|
115
|
0
|
115
|
0
|
0
|
|
1
|
1
|
1
|
0
|
1
|
0
|
0
|
Case detection and reporting
Individual suspected for COVID-19 at health post or health facility level will be communicated to Rapid Response Team (RRT) of that catchment. The RRT will report to laboratory for sample collection and sample will be collected and transported to testing laboratory. Result will be communicated to the Regional Health Bureau and the Federal Ministry of Health, EPHI. The Regional Health Bureau is responsible to communicate result back to the RRT for necessary action.
From the Regional Health Bureau laboratory-based surveillance data, up to July 30, 2020, there were 150 contacts, 115 suspects and 521 risk group tested for COVID-19-from Nekemte town. Positive result was found only from risk group testing, 10/521 (2%). From Shambu town 1 suspect and 114 risk groups were tested within the same time period, none of which turned positive.
Surveillance attributes
Data Quality
There is no consistency in reporting of date of testing, either Gregorian or Ethiopian calendar is in use. Individual suspected for COVID-19 can be tested several times without being recognized, as there is no control mechanism for repeated testing except for those under treatment.
Simplicity
Of the visited, 75% health facilities considered the variables on the report are simple to understand. Half (50%) of the health facilities reported that means of data collection is convenient for them.
Acceptability
More than half, 75% of the health facilities in both towns reported they have complaint on the surveillance system. The main reasons for complaint are lack of support from authority (100%), a lot of reportable variables (67%) and internet interruption (67%).
System usefulness
The laboratory-based surveillance is being used for contact tracing and case management. Data analysis was not being done at both towns to identify the most at-risk group and location. The health authorities in both towns are not using surveillance data for any decision making.
{kind=link}